Advances in Clinical Medicine
Vol.1 No.3(2011), Article ID:397,11 pages DOI:10.4236/acm.2011.13008
Snake Bites in Taiwan
1Department of Emergency Medicine, Kuang-Tien General Hospital, Taichung
2General Education Center, National Chi Nan University, Nantou
3Department of Health-Business Administration, Hungkuang University, Taichung
Email: juanchiwen@yahoo.com.tw
Received: Oct. 15th, 2011; revised: Nov. 13th, 2011; accepted: Dec. 3rd, 2011.
ABSTRACT:
Located at the juncture of tropical and subtropical regions, Taiwan has a warm and humid climate with abundant precipitation and food, which coupled with the island’s diverse vegetation and landscape, makes it a suitable environment for many snake species. Among these, there are six kinds of poisonous snake with epidemiological significance. Three species induce hemorrhagic symptoms (Trimeresurus mucrosquamatus, TM; Trimeresurus stejnegeri, TS; and Deinagkistrodon acutus, DA); two species induce neurotoxic symptoms (Naja naja atra, NA; and Bungarus multicinctus, BM); the other species induces hemorrhagic and neurotoxic symptoms (Vipera russelli formosensis. VR).The hemorrhagic venom causes disorders of the clotting cascade such as prolonged bleeding, primary fibrinolysis and disseminated intravascular coagulopathy. The neurotoxic venom provokes respiratory distress from weakened respiratory muscles, blurred vision, diplopia, dysarthria, dysphagia, dysphonia and paralysis of extremity muscles. The mixed envenomation manifests as a combination of neurotoxic and hemorrhagic effects previously described, as well as rhabdomyolysis and acute renal failure. The identification of snake species is important if antivenom is to be used. However, the species is not ably identified if the patient or companion fails to see or catch the responsible snake. Although these unidentifiable snakes could be non-venomous, venomous species are not uncommon. Therefore, guidelines for snakebite identification based on clinical symptoms and laboratory analysis is important to improve clinical diagnosis of snakebites. In Taiwan, T. stejnegeri bites are the most common. The second is T. mucrosquamatus. Naja naja atra is the third, Bungarus multicinctus is the forth and Vipera russelli formosensis is the fifth. Deinagkistrodon acutus is the least. Bites by Deinagkistrodon acutus and Vipera russelli formosensis generally occur in the south and east parts of the island. Aggressive antivenom treatment can reduce snakebite mortality rate, but for Bungarus multicinctus bites, maintaining the patient’s airway and supporting their ventilation is vital to reducing mortality rate in addition to antivenom treatment. For dry bites or no envenomation, the patient should be observed for at least 6 - 12 hours before discharged. The emergency physician should determine the severity of envenomation and predominate venom activity before decide what type of antivenin to administer, how much, and over what period. History of exposure, local effect and systemic syndromes of envenomation, progression of symptoms and signs, laboratory data obtained in emergency department should guide the decision for antivenom therapy. The freeze-dried antivenom was diluted with 50 - 100 mL of normal saline and infused intravenously for half to one hour. The poisonous snake bites in the latter 4 hours to give the effect to be best, surpasses 8 hours only then to inject the effect to be bad. The dosage most toxicologists used for treating pediatric patients with snakebites was the same as that for adults. In general, 6 - 12 vials of antivenom against neurotoxic venom were used for Naja atra bite and 2 - 4 vials for Bungarus multicinctus; 1 - 2 vials of antivenom against hemotoxic venom was used for Trimeresurus stejnegeri and 2 - 4 vials for Trimeresurus mucrosquamatus; 2 - 4 vials of anti-Deinagkistrodon acutus were used for Deinagkistrodon acutus and 2 - 4 vials of anti-Vipera russelli formosensis were used for Vipera russelli formosensis bite. During the infusion, the blood pressure, consciousness and skin reaction were evaluated. Keeping the varied clinical manifestations of snake bite in mind is important for effective management. Ready availability and appropriate use of antivenin, close monitoring of patients and institution of ventilatory support, all help reduce mortality.
Keywords: Snake Bites; Antivenin; Hemorrhagic Venom; Neurotoxic Venom
毒蛇咬伤台湾经验
阮祺文1,2,3
1光田医疗社团法人光田综合医院急诊医学部,台中
2国立暨南国际大学通识中心,南投
3弘光科技大学健康事业管理系,台中
Email: juanchiwen@yahoo.com.tw
摘 要:
台湾地处亚热带,地形多高山、丛林,气候温暖潮湿,是毒蛇生长繁殖的最佳环境。其中有6种毒蛇的咬伤较为常见且常有严重的临床症状,较有流行病学上的意义,它们是赤尾鲐(Trimeresurus stejnegeri)、龟壳花(T.mucrosquamatus)、眼镜蛇(Naja naja atra)、雨伞节(Bungarus multicinctus)、百步蛇(Deinagkistrodon acutus)、锁蛇(Daboia russelli formosensis)(2)。赤尾鲐、龟壳花及百步蛇咬伤主要以出血症状为主,一般称之出血性毒蛇。眼镜蛇和雨伞节咬伤因其具神经毒性,故称之为神经性毒蛇。锁炼蛇在动物实验及临床上兼具神经及出血症状,另外归为两者兼有之毒蛇。出血性毒毒素可造成咬伤处肿胀、淤血、疼痛;严重时并可导致血凝不全、全身性出血等症状。神经性毒毒素可以作用于运动神经与肌肉接合处,而造成横纹肌不收缩,迅速导致呼吸麻痹。混合性毒毒素具有神经毒性、溶血、横纹肌溶解及肾毒性等症状。赤尾鲐的咬伤是台湾最常见的毒蛇咬伤,龟壳花次之,眼镜蛇咬伤占第三位,不过赤尾鲐咬伤有集中在台湾中部的倾向,雨伞节咬伤占第四位,锁炼蛇占第五位、百步蛇咬伤个案在六大毒蛇中反而最少,不过锁炼蛇及百步蛇咬伤主要以台湾东南部为主[4,22-23]。一般毒蛇咬伤后在4~6小时即会有症状出现,此时应尽速给予正确的抗蛇毒血清(量及种类),雨伞节咬伤尚需考虑插管使用呼吸器维持呼吸,若4~6小时内未出现症状,则最好观察6~12小时确定无症状再离院,无症状的毒蛇咬伤并不需给予抗蛇毒血清治疗,仅需一般症状治疗。蛇咬时应保持冷静,辨别蛇种及蛇的大小,并注意有无听到嘶嘶的喷气声以帮助医护人员诊断。抗蛇毒血清使用的剂量依咬伤的严重度、病人体重及咬伤后的时间长短给予不同的剂量,根据大多数毒物专家建议大人与小孩毒蛇咬伤应给予相同剂量,饭匙倩咬伤为6~12瓶、雨伞节咬伤为2~4瓶、龟壳花咬伤为2~4瓶、赤尾鲐咬伤为1~2瓶、百步蛇咬伤为2~4瓶、锁链蛇咬伤为2~4瓶,抗蛇毒血清以静脉滴注30~60分钟,毒蛇咬伤后4小时内给予效果最好,超过8小时才注射效果较差。急诊医护人员应根据毒蛇咬伤的病史,临床进展的症状及实验室的检查报告来决定适时给予何种抗蛇毒血清的注射量,滴注期间应密切注意病患各种生理现象的变化,才能降低毒蛇咬伤的死亡率。
收稿日期:2011年10月15日;修回日期:2011年11月13日;录用日期:2011年12月3日
关键词:毒蛇咬伤;抗蛇毒血清;出血性毒毒素;神经性毒毒素
1. 引言
台湾地处亚热带,地形多高山、丛林,气候温暖潮湿,是毒蛇生长繁殖的最佳环境。「蛇」是一种细长且没有四肢的爬虫类变温动物,蛇是由蜥蜴演化而来,蜥蜴类的舌头单一不分叉,但蛇类的舌头细长而分叉,蛇常常吐舌头,其目的是将空气中的化学物质黏附在舌头上,以便收回舌头插入杰克逊氏器再传送至大脑分辨,便可察觉出前面有什么东西,因此蛇类具有非凡的嗅觉,但听觉不好视力也差。不过蛇类的腹部感觉神经非常敏感,可查知地上100英尺远的震动,且攻击速度很快,每秒可达8英尺,但是每次攻击的距离不会超过其身长的一半,只要不太靠近即不易被蛇咬。根据既有的资料,全台湾共有62种蛇,其中有毒的蛇23种(包括海蛇9种,陆上毒蛇14种)。毒蛇的头大部分呈三角形,在三角形的两个底角部份是毒腺分泌毒液演化膨大的结果,但雨伞节的头是椭圆形并非三角形,仍是不折不扣的毒蛇,毒蛇的毒液主为消化食物之用,次为防卫攻击猎物之用,当毒蛇咬囓时,上下颔相互挤压毒液囊而将毒液经由毒牙注入猎物,毒牙分为管牙和沟牙,管牙呈中空管状如注射针样,因此咬伤时易有明显的毒牙痕,蝮蛇科的赤尾青竹丝、龟壳花、锁链蛇等的毒牙为管牙。沟牙较小且大部分埋在齿龈内,沟缘相接成沟,毒液再经此沟注入猎物体内,咬伤时不易见明显毒牙痕,蝙蝠蛇科的雨伞节及饭匙倩属之[1]。根据疾病管制局(原预防医学研究所)从抗蛇毒血清的使用上所作粗略估计,每年约有1000个人次被毒蛇咬过。其中有6种毒蛇的咬伤较为常见且常有严重的临床症状,较有流行病学上的意义,它们是赤尾鲐(Trimeresurus stejnegeri)、龟壳花(T.mucrosquamatus)、眼镜蛇(Naja naja atra)、雨伞节(Bungarus multicinctus)、百步蛇(Deinagkistrodon acutus)、锁炼蛇(Vipera russelli formosensis)[2]。赤尾鲐、龟壳花及百步蛇咬伤主要以出血症状为主,一般称之出血性毒蛇。眼镜蛇和雨伞节咬伤因其具神经毒性,故称之为神经性毒蛇。锁炼蛇在动物实验及临床上兼具神经及出血症状,另外归为两者兼有之毒蛇。抗蛇毒血清大体上即根据上述分颣来分别制备,目前市面上有三种血清,它们是抗出血性蛇毒血清(对抗赤尾鲐及龟壳花)、抗神经性蛇毒血清(对抗眼镜蛇及雨伞节),抗百步蛇血清及抗锁炼蛇蛇毒血清[3]。这六种常见的毒蛇依照毒液的性质可大略分为三类,兹介绍于后[3]:
1. 出血性毒:被咬后伤口肿胀、疼痛、及出血,具有此类作用毒液的毒蛇均属蝮蛇科响尾蛇亚科(Crotalinae, Viperidae)。其共同特性是在攻击前会先卷缩且抖动尾巴;另一特点是在其眼睛与鼻孔间有一小孔称为颊窝(Loreal pit),其中的薄膜上布满神经,对热特别敏感,在黑暗中可感受到温血动物体表的辐射热而进行攻击,有名的响尾蛇飞弹即依照此原理设计并命名。出血性毒蛇所含的毒素主要有phsopholipase A2(龟壳花)、fibrinogenase(龟壳花)、抗凝血醣蛋白、促凝血醣蛋白(百步蛇、青竹丝)等。此等毒素可造成咬伤处肿胀、淤血、疼痛;严重时并可导致血凝不全、全身性出血等症状。高浓度的出血性毒蛇毒素也有可能导致促进凝血之作用。
2. 神经性毒:其毒素为小分子的蛋白质或多胜类。神经性毒蛇之毒素主要有 cobrotoxin(眼镜蛇)、心脏毒素cardiotoxin (眼镜蛇)、phospholipase A(眼镜蛇)、α-及β-bungarotoxin(雨伞节)等毒素。此种毒素可以作用于运动神经与肌肉接合处,而造成横纹肌不收缩,迅速导致呼吸麻痹。此类蛇属蝙蝠蛇科(Elapidae)。
3. 混合性毒:混合性毒蛇之毒素则甚为复杂,包括凝血、溶血毒、神经毒、心脏毒(海蛇)、肌肉毒(海蛇)等,因此可造成神经毒性与出血症状此类蛇属蝮蛇科的蝮蛇亚科(Viperinae, Viperidae)[4-5]。
但毒蛇之所以会分泌毒液主要是为了觅食、消化食物以及抵抗敌人[6];因此,经过长期演化过程,毒蛇之毒液(蛇毒)的成份事实上相当的复杂,其致毒的成份除了致死或麻痹猎物的主要毒性成份之外,常另有多种蛋白质脢,可以破坏局部组织或某些主要器官,甚至连其主要毒性成份的致毒作用都具多变性,例如锁炼蛇蛇毒中含量最多的phospholipaseA2,根据研究,就具有神经毒性、溶血、横纹肌溶解及肾毒性等[7-8]。因此,虽有上述出血性或神经性的毒性分类,但当病人被咬伤时,可能无法抓到蛇、没有看到或无法分辨其种类,在诊断及治疗上造成相当大的困扰。毒蛇咬伤时,毒蛇毒液注到伤口量的多寡、毒性成份的变异以及病人本身的身材大小及疾病状况等,都严重影响中毒的程度3,进而影响到咬伤之后的临床表现,在咬伤中毒早期甚至后期临床症状可能都仍相当混淆,无法作正确的蛇种诊断,无法给予最正确的血清治疗[3]。国外有人报告[9-10],有1~3成毒蛇咬伤其实只是干咬(即没有注入毒液)或超过60%不知被何种蛇咬伤,中毒量也常无法评估,治疗时常无法决定正确的血清及治疗量。
回顾国内外毒蛇咬伤之流行病学相关文献:各国均有相关之文献纪录,例如东南亚的泰国[11],非洲的南非[12]、巴布亚纽几内亚[13]及澳洲[14]等国家。而在美国每年约将近有8000人被毒蛇咬伤,约占蛇类咬伤事件的2成[15-17],其中约有12~15位受害者因此死亡[18-19]。美国地区多数毒蛇咬伤事件发生在4~10月[20]且从事户外活动者居多。而台湾地区除了百步蛇、锁炼蛇分布较偏重南部及东部山区之外,其它四种毒蛇在全台各地都可见。但毒蛇咬伤的流行病学长久以来只有少数研究性数据,但其数据不是年代久远[21],即少数研究单位及医院自行研究[22-23]。其结果均属区域性的数据,全国而较完整的资料却一直没有相关的文献。
赤尾鲐的咬伤是台湾最常见的毒蛇咬伤,龟壳花次之,眼镜蛇咬伤占第三位,不过赤尾鲐咬伤有集中在台湾中部的倾向,雨伞节咬伤占第四位,锁炼蛇占第五位、百步蛇咬伤个案在六大毒蛇中反而最少,不过锁炼蛇及百步蛇咬伤主要以台湾东南部为主[4,22-23]。
2. 赤尾鲐(Trimeresurus stejnegeri, Bamboo viper)
赤尾鲐因其身体绿色,尾巴红色,故又名为赤尾青竹丝、竹仔蛇,若尾巴是绿色,则为无毒的青蛇,两者的区别在于是否有“赤尾”。赤尾鲐头呈三角形,有颊窝,颊窝为介于眼与鼻之间的凹窝,左右各一,内有血管与三叉神经分布,是温度探测器,可侦侧周遭环境细微温度的改变,藉以搜寻小型哺乳类动物身上的体温并加以捕食,口内有一对大管牙,体长约50公分,咬伤后有明显毒牙痕,体色极具掩护作用属树上蛇,为出血性毒,作用机转仍不明,主要毒素成份有出血成份(Hemorrhagic factors HR1和HR2)、凝血成份(platelet aggregoserpentin)、抗凝血成份(platelet aggregation inhibitor, 5’一核甘酸分解酵素),高浓度呈现促凝血作用(似Thrombin作用),低浓度则具溶血作用,分布于中国大陆东南部及台湾,遇到目标会凶猛的攻击,被咬伤后患处肿痛、出血、起水泡,在台湾为分布最广的毒蛇,数量最多且是咬伤率最高的一种,但因其毒液量少,致死率低[23-25]。(图1~5)

Figure 1. Trimeresurus stejnegeri bites the Figure 2 patient
图1. 咬伤员者被抓到之赤尾鲐

Figure 2. Trimeresurus stejnegeri bites the forearm of the patient
图2. 被图1赤尾鲐咬伤员者之前臂

Figure 3. Swelling forearm bitten by Trimeresurus stejnegeri
图3. 被赤尾鲐咬伤员者前臂肿胀

Figure 4. Swelling blister foot bitten by Trimeresurus stejnegeri
图4. 被赤尾鲐咬伤员者足背肿胀起水泡

Figure 5. Swelling forearm bitten by Trimeresurus stejnegeri
图5. 被赤尾鲐咬伤员者前臂肿胀
3. 龟壳花(Trimeresurus mucrosquamtus, Taiwan habu)
龟壳花体背中央有一行较大状似龟壳之暗茶色斑块,体两侧也各有一列较小状似龟壳之暗茶色斑块,上下相连且左右弯曲呈波浪状斑纹,头大呈三角形,又名牛角蛇,体长约95公分,栖息于荫凉处,夜间较活跃,是台湾常见毒蛇中攻击性最强者,有颊窝,口内有一对大管牙,咬伤有明显毒牙痕,分布于台湾、中国大陆南部、寮国、越南、缅甸,喜居人类居住的地方,故在住屋附近被咬伤者居多,咬伤率仅次于赤尾鲐,属出血性毒,主要毒素成份有phospholipase A2,Fibrinogenase及platelet aggregoserpentine。Phospholipase A2作用分解磷脂质影响细胞膜渗透作用使红血球变形,破坏血管内皮细胞。Fibrinogenase作用为破坏Fibrinogen,具有出血作用,platelet aggregoserpentine促进血小板凝集具有凝血作用。咬伤后患处肿痛、瘀血、起水泡及血泡[23,26,27]。(图6~7)
4. 百步蛇(Agkistrodon acutus, five pace snake)
百步蛇身体两侧各有一列倒三角形具黑边深棕色斑纹排列,头大呈三角形,嘴尖向上翘,头状似虌头,故又名山谷虌,体长约95公分,体重约500~1200公克是台湾地区毒蛇中体形最大的一种,具有中度的攻击性,因数量急速减少被列为保育的野生动物,有颊窝,口内有一对大管牙,可长达3~4公分,属出血性毒,毒性物质有ADPase、5’-nucleotidase、phospholipase A2及fibrinogenase,其中ADP ase具有明显抑制血小板凝集功能,导致出血倾向。咬伤后患处肿痛、瘀血、起血泡,症状和赤尾鲐、龟壳花等出血性毒蛇相似,唯一不同是血小板会明显减少,可资区别,故治疗除给予抗蛇毒血清外尚需补充血小板,百步蛇咬伤以前是台湾毒蛇咬伤致死率最高的一种,但由于抗蛇毒血清的发达及血小板制剂的补充,致死率已大大地降低[23,28,29]。(图8~9)

Figure 6. Trimeresurus mucrosquamtus bites the Fig 7 patient
图6. 咬伤员者被抓到之龟壳花

Figure 7. Swelling forearm bitten by Trimeresurus stejnegeri
图7. 被图6龟壳花咬伤员者前臂肿胀

Figure 8. The patient dorsum pedis swelling blood blister bitten by Agkistrodon acutus
图8. 被百步蛇咬伤员者足背肿胀起血泡

Figure 9. When mountaineering, the contact lenses fall in the thick patch of grass, when pursuing, is attacked the right eyeball by Agkistrodon acutus, early evisceration for the penetrating ocular injury by Hualian Buddhist Tzu-Chi General Hospital urgent operation (Hualian Buddhist Tzu-Chi General Hospital to provide)
图9. 登山时隐形眼镜掉落草丛中,在找寻时被草丛中的百步蛇攻击右眼球,经花莲慈济医院紧急开刀取出咬伤眼球,致右眼失明(慈济医院提供)[30]
5. 饭匙倩(Naja naja atra, Taiwan cobra)
饭匙倩背部暗褐色,腹部偏白,头部有一条较宽的黑白环纹,乍看似戴眼镜,故又名为眼镜蛇,惊怒时上身直立,颈部变扁平犹如饭匙并发出喷气声,平地较多见,不爱活动,夜间出来,对黑色敏感,攻击性强,动作迅速准确,头呈三角形无颊窝,口内有对细沟牙长约1~3 mm,咬伤后不易见到毒牙痕,分布于泰国、中国大陆南部、越南东部及台湾,虽归类为神经性毒蛇,但其毒素成份神经毒Cobrotoxin仅占20%,其余80%为心脏毒素Cardiotoxin,此心脏毒素为细胞毒性(Cytotoxin),咬伤后很快造成患处极度疼痛、肿胀并局部组织变黑坏死,故眼镜蛇咬伤后除了给予蛇毒血清外,常需植皮或补皮瓣。根据研究,台湾东部的眼镜蛇的毒性是西部眼镜蛇的二倍,故在
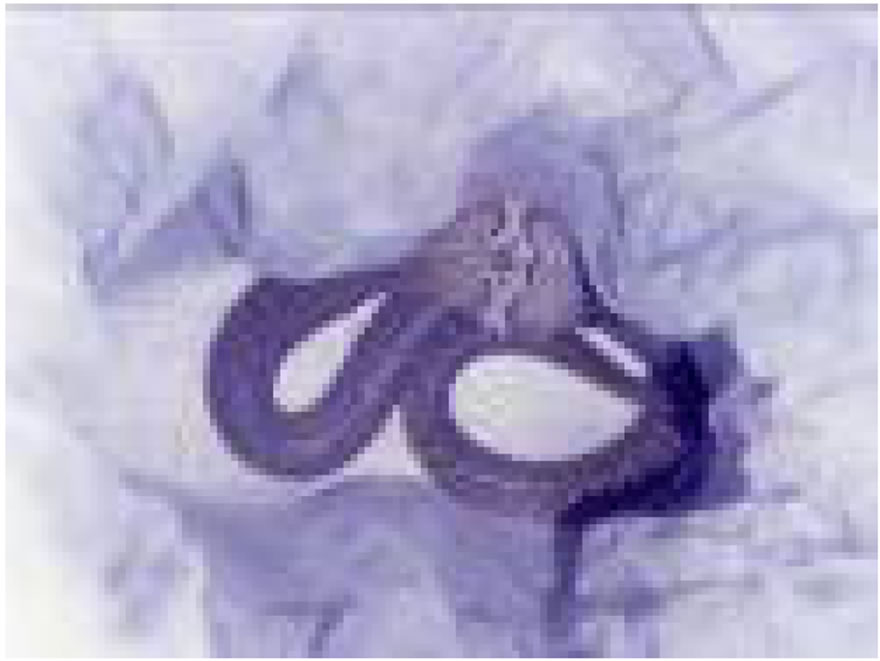
Figure 10. Naja naja atra bites the Figure 11 patient
图10. 咬伤病患被活抓的饭匙倩

Figure 11. The patient dorsum pedis swelling necrosis bitten by Naja naja atra
图11. 被饭匙倩咬伤足背,足背组织肿胀坏死

Figure 12. After surgical debridement to remove the patient dorsum pedis necrotic tissue
图12. 足背组织肿胀坏死,经扩创处理,清除坏死组织

Figure 13. The patient receive split-thickness skin grafts surgery
图13. 足背坏死组织经扩创处理,再施以分层植皮手术

Figure 14. Naja naja atra bites the Figure 15 patient
图14. 咬伤病患被打死的饭匙倩
台湾东部被眼镜蛇咬伤其抗蛇毒血清亦需加倍给予[4,23,31-34]。(图10~30)

Figure 15. Inappropriate herb drug treatment for snakebite wound to increase the wound infection risks
图15. 被图14饭匙倩咬伤足背,用中草药治疗徒增伤口感染的风险

Figure 16. The patient dorsum pedis swelling necrosis bitten by Naja naja atra
图16. 被饭匙倩咬伤足背,足背组织肿胀坏死

Figure 17. The patient receive split-thickness skin grafts surgery
图17. 足背坏死组织经扩创及植皮手术治疗
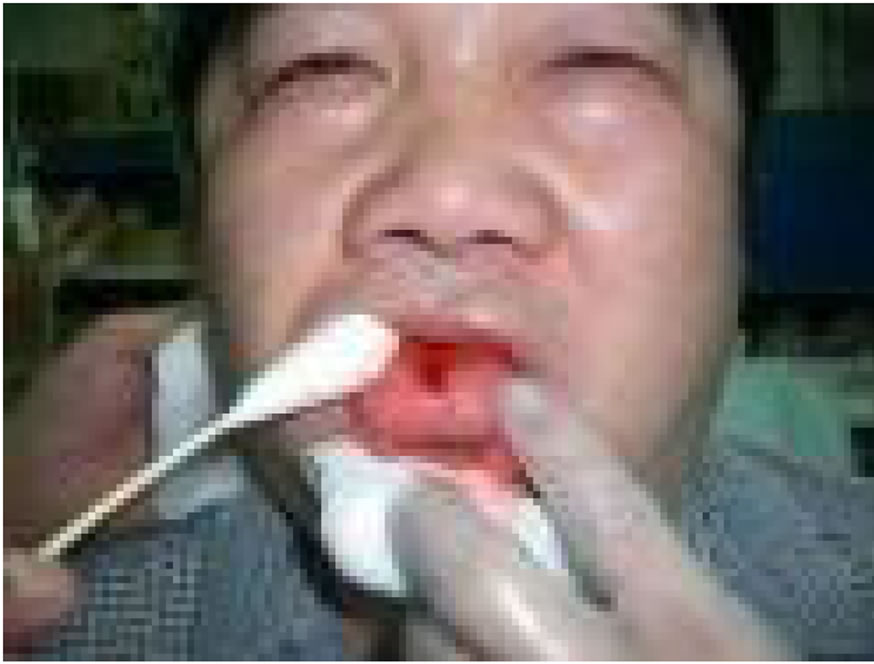
Figure 18. Bloody fluid exuding from fang punctures on the dorsum of tongue.
图18. 表演与饭匙倩接吻之工作者,不慎被饭匙倩咬伤舌头

Figure19. Central tongue swelling, ecchymosis and myonecrosis even after 6 vials antivenom .
图19. 虽然施打饭匙倩6瓶抗蛇毒血清,病患舌头中央仍呈现泛黑坏死状
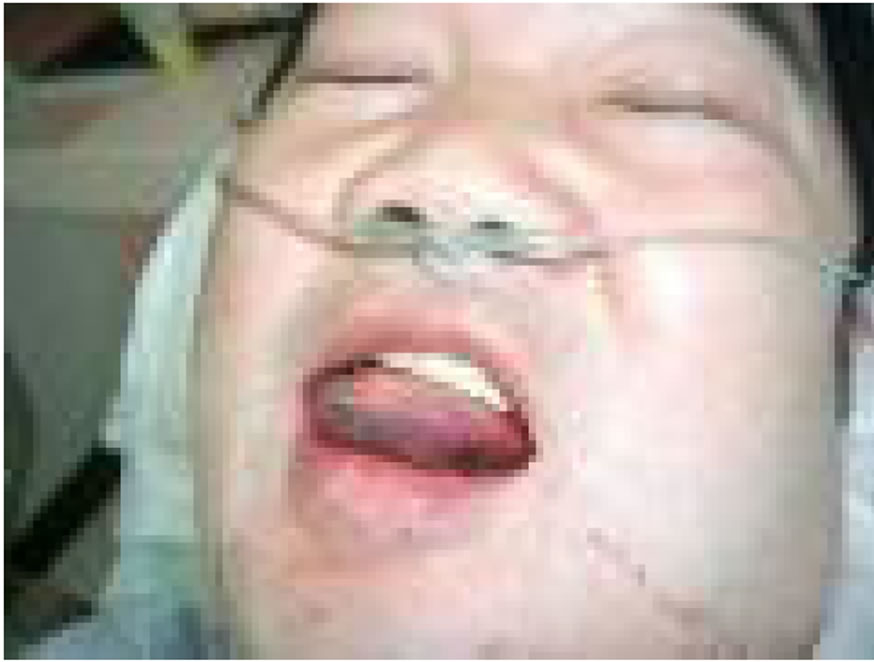
Figure 20. 2 hours later, tongue base swelling, ecchymosis and myonecrosis.
图20. 2小时后舌底也呈现泛黑坏死状
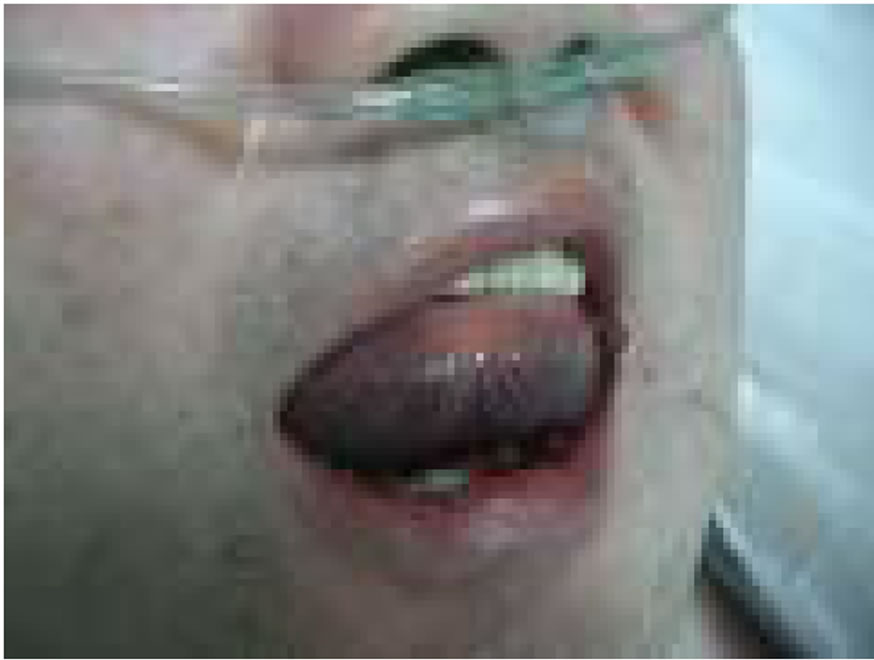
Figure 21. 2 hours later, nearly the whole tongue swelling, ecchymosis and myonecrosis.
图21. 2小时后舌底及舌尖皆呈泛黑坏死状

Figure 22. 2 hours later, the whole tongue swelling, ecchymosis and myonecrosis, tongue excision is considered.
图22. 2小时后,整个舌头皆呈现泛黑坏死状

Figure 23. 4 hours later tongue tip restores the blood follow
图23. 4小时后病患舌尖先恢复血循颜色

Figure 24. 2 hours later. all the tounge circulation restores.
图24. 2小时后病患舌头大部份恢复血循颜色
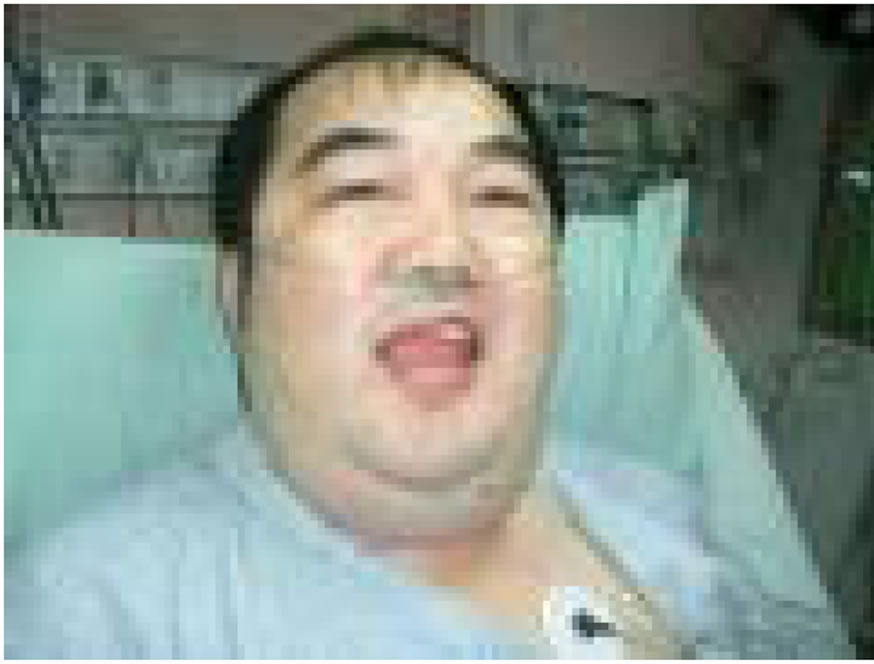
Figure 25. Good viability and mobility after quick antivenom treatment. and goog blood supply of tongue
图25. 2小时后病患整个舌头都恢复原状,病患复原迅速,应归功于尽早给予足量的抗蛇毒血清及舌头血液循丰富所致

Figure 26. Unknown small snake to bite the Fig19 patient is caught
图26. 咬伤病患足背被抓到之不知名小蛇

Figure 27. Emergency room nurse plays tricks on the small snake startled anger upper body erectness by the bamboo stick, the small snake is Naja naja atra
图27. 急诊室护士以竹棒戏弄小蛇惊怒上身直立,颈部变扁平始知饭匙倩

Figure 28. The patient dorsum pedis swelling pain bitten by small Naja naja atra
图28. 被饭匙倩小蛇咬伤足背,足背肿胀疼痛

Figure 29. The snake to bite the Fig19 patient is caught and beheaded immediately, the snake is known as Naja naja atra by back black and white concentric pattern
图29. 咬伤病患右手被抓到迅即被砍头处决之蛇,由背部黑白环纹得知是饭匙倩

Figure 30. The patient right hand swelling pain bitten by Naja naja atra
图30. 被饭匙倩咬伤右手,右手肿胀疼痛
6. 雨伞节(Bungarus multicinctus, Taiwan banded krait)
雨伞节因全身有黑宽白窄相间的横带,故又名为百节蛇,该蛇喜栖水边,性温顺,属夜行性蛇,头小而圆不呈三角形,无颊窝,口内有一对大沟牙,二对小沟牙,分布于缅甸、中国大陆南部及台湾,属神经毒(Bungarotoxins),作用于神经肌肉接合处,进而阻断神经传导使得横纹肌不收缩,导致呼吸麻痹,因此当病患出现眼睑下垂(Ptosis)或胸闷时,应尽速给予抗蛇毒血清并考虑插管使用呼吸器维持呼吸,雨伞节咬伤后,伤口并无明显肿痛症状,故常让患者忽略而未就医,待觉得昏昏欲睡时,常在30分至2小时内即演变成致命的呼吸衰竭,目前是台湾毒蛇咬伤死亡率最高的,可高达24%,因此若被雨伞节咬伤,应尽速送医观察治疗,若有呼吸衰竭现象则尽速插管使用呼吸器并给予抗蛇毒血清,常可化险为夷,挽回一命[23,35,36]。(图31~35)

Figure 31. Bungarus multicinctus bites the Figure 32 patient right middle finger
图31. 咬伤病患右手中指被抓到之雨伞节

Figure 32. The patient right hand bitten by Naja naja atra not obvious symptom is noted
图32. 病患右手中指被雨伞节咬伤,伤口无明显症状

Figure 33. This drowsy patient tries to make an effort to open the eye, the forehead obviously obvious wrinkle, but the eye actually does not open is the typical ptosis symptom
图33. 病患呈现嗜睡状态,请其用力张开眼睛,额头可见明显皱纹,但眼睛却张不开是典型的眼脸下垂症状

Figure 34. This drowsy patient accepts the intubation and 2 vials antivenom treatment immediately
图34. 病患随即接受插管及2瓶抗蛇毒血清治疗

Figure 35. Next day, after antivenom treatment, this patient may open the eye freely and the breath is smooth without ventilatory support
图35. 隔天,病患毒液被抗蛇毒血清中和,眼脸下垂及呼吸急竭情况改善,随即拔管,病患可自由张开眼睛,呼吸顺畅
7. 锁链蛇(Vipera russelli formosensis, Russell’s pit viper):
锁链蛇体背有三纵列锁链状(非龟壳状)斑纹,故称为锁蛇或锁链蛇,常被误认为龟壳花,头呈三角形无颊窝,常见于台湾东南部山区、广东、印度喜马拉雅山,性情凶猛,常在夜间活动,具攻击性,会如眼镜蛇般发出嘶嘶的喷气声,其毒素有出血性及神经性两种混合毒素,毒素甚为复杂,有pro-coagulation factors V和X actiuators,protease inhibitor及phospholipase A2,会引起凝血反应,耗损其他凝血因子形成血栓,阻塞血管,导致多发性血栓血管阻塞病变,引起全身扩散性血管内凝血病变(DIC)。咬伤后局部肿胀轻微,主要以出血及溶血症状为主,皮下多处瘀血及紫斑,并常导致急性肾衰竭及血小板减少,尽早给予锁链蛇抗蛇毒血清2~4剂治疗可有效改善凝血机能障碍,但对肾机能伤害改善有限,常需进行血液透析治疗[37-40]。(图36~37)

Figure 36. Vipera russelli formosensis
图36. 台湾的锁链蛇

Figure 37. A middle-aged man is bitten by Vipera russelli formosensis the right toe and expired in. Hengchun Hospital even after antivenom treatment immediately
(Hengchun Hospital to provide)
图37. 一恒春中年男子被锁链蛇咬伤右脚趾送医不治死亡。恒春医院提供
8. 毒蛇咬伤的处理:
1) 保持镇静:被毒蛇咬伤约有1/3的机会是干咬,亦即虽被毒蛇咬伤,但毒液来不及注入人体,有2/3的机会是有毒液注入人体,人体中毒的反应取决于蛇毒的量及蛇种,蛇越大贮毒量也越多,中毒反应也越厉害,因此蛇咬时应保持冷静,辨别蛇种及蛇的大小,并注意有无听到嘶嘶的喷气声以帮助医护人员诊断。(图38)
2) 移除肢体上束缚物:青竹丝、龟壳花、百步蛇、饭匙倩等毒蛇咬伤,很容易造成肢体肿胀坏死,因此肢体若有任何束缚物如戒指、手表、手环等应尽速移除,以免肿胀后束缚物不易移除并压迫到局部的血液循环,加速肢体坏死,亦不能冰敷及使用止血带,因肿胀的肢体居部血液循环变差,冰敷或使用止血带将造成肢体局部血液循环更差。(图39~41)
3) 不要切开伤口,不要用口吸毒液:除非随身携带吸血器,在毒蛇咬伤后立即使用30分钟,约可吸出30%左右的毒液,否则不要用口吸以免口内有伤口成为第二位受害者;毒蛇咬伤,毒液注入深部组织迅速进入体内淋巴循环再进入血液循环,故在紧急状况消毒不完全下切开伤口并无法将毒液清出,反而增加感染的危险。
4) 由于毒蛇咬伤人体后30分钟在血液中即可达最高浓度,因此被咬伤肢体应尽可能保持低于心脏的位置,并尽速以弹性绷带作压迫性包扎,再以夹板或三角巾固定患肢以减缓毒液进入人体的速度,并不要

Figure 38. The same side bitten by the poisonous snake not suitable intravenous injection treatment avoids worsening the tissue swelling
图38. 被毒蛇咬伤同侧肢体部位不宜静脉注射治疗以避免恶化组织肿胀

Figure 39. The site bitten by the poisonous snake not to be suitable to use the tourniquet, avoids misinterpreting to be the venom create swelling or the tourniquet create swelling, confuses whether to give antivenom treatment or not
图39. 被毒蛇咬伤部位不宜用止血带,以避免误判是毒液造成肿胀或止血带造成肿胀,增加是否给予抗蛇毒血清治疗之困扰

Figure 40. The middle finger bitten by the snake, with the red adhesive tape bundle middle finger, cyanosis is noted
图40. 被蛇咬伤中指,用红色胶带捆绑中指,致中指呈现血循不良状态

Figure 41. The red adhesive tape detachment, the middle finger restores the blood follow and non-venom response symptom
图41. 迅速将红色胶带移除,中指恢复血循颜色纯系干咬,并无毒液反应症状
喝酒以免促进血液循环,加速毒液吸收,尽速送医诊治,并避免先行给予中草药敷治伤口,以免增加伤口的感染机会。
5) 一般毒蛇咬伤后在4~6小时即会有症状出现,此时应尽速给予正确的抗蛇毒血清(量及种类),若4~6小时内未出现症状,则最好观察6~12小时确定无症状再离院,无症状的毒蛇咬伤并不需给予抗蛇毒血清治疗,仅需一般症状治疗。
6) 血清治疗:卫生署疾病管制局是国内唯一制造抗蛇毒血清的机构,目前生产抗蛇毒血清的种类有抗雨伞节及饭匙倩蛇毒混合血清、抗龟壳花及赤尾鲐蛇毒混合血清、抗百步蛇蛇毒血清及抗锁链蛇蛇毒血清等四种,台湾抗蛇毒血清是以胃蛋白酵素消化法精制纯化的血清,以Fab2形式使用,效价极高,每瓶血清所含效价在1000田中单位(U)以上。制造方式是以减毒性的蛇毒,分多次小剂量注入马匹体内,使马产生免疫力,再抽取马血,经过重重安全及效价试验,制成抗蛇毒血清,每瓶抗蛇毒血清平均有1200田中单位,每一田中单位可中和体重12到14公克老鼠之最低致死剂量,抗蛇毒血清使用的剂量依咬伤的严重度、病人体重及咬伤后的时间长短给予不同的剂量,根据实验室的蛇毒中和试验建议给予剂量,饭匙倩咬伤为6~12瓶、雨伞节咬伤为2~4瓶、龟壳花咬伤为2~4瓶、赤尾鲐咬伤为1~2瓶、百步蛇咬伤为2~4瓶、锁链蛇咬伤为2~4瓶,抗蛇毒血清以静脉滴注30~60分钟,毒蛇咬伤后4小时内给予效果最好,超过8小时才注射效果较差。但根据临床经验,咬伤经过7~10天再给予正确血清仍有明显效果,不宜放弃。小孩毒蛇咬伤,因小孩血液量较大人为少,相对的毒液浓度也较高,故抗蛇毒血清给予剂量与大人相同,因毒性的大小取决于注入毒液之分子量大小(Molar size)而非被咬伤者身体的大小[4,41-46]。抗毒血清使用前须先作过敏试验。方法是取1 U作皮肤试验(将1000 U抗毒血清稀释到10 ml之稀释液,再取其中1 ml稀释液再加入稀释液成为10 ml,取0.1 ml)。如30分钟内局部产生轮状浮肿,且周围起红晕者,视为阳性;否则为阴性。如患者皮肤试验为阳性反应,且确实需抗毒血清之治疗,可以先行注射抗过敏药剂并减慢注射速度至30分钟至2小时;同时准备急救设备与急救药物在旁,以便发生过敏性休克时可救急。
参考文献 (References)
[1] 毛寿先, 殷凤仪. 台湾常见陆地毒蛇简介[J]. 台湾省立博物馆, 1990.
[2] Y. Sawai. Snakebites on Taiwan. The Snake, 1969, 1: 9-18.
[3] 洪东荣. 台湾常见的毒蛇及咬伤之治疗[J]. 毒药物季刊, 行政院卫生署临床毒药物咨询中心, 1996.
[4] B. L. Miao, R. J. Huang, M. S. Hu, et al. Venomous snakebite in Taiwan (1988-1991). Chinese Journal of Public Health (Taipei), 1995, 14: 455-460.
[5] D. Z. Hung. Taiwan’s venomous snakebite: Epidemiological, evolution and geographic differences. Transactions of the Royal Society of Tropical Medicine and Hygiene, 2004, 98(2): 96-101.
[6] B. K. Nelson. Snake evenomation: Incidence, clinical presentation and management. Medical Toxicology, 1989, 4(1): 17-31.
[7] D. A. Warrell. Snake venoms in science and clinical medicine 1. Russell’s viper: Biology, venom and treatment of bites. Transactions of the Royal Society of Tropical Medicine and Hygiene, 1989, 83(6): 732-740.
[8] R. N. H. Pugh, R. D. G. Theakston. A clinical study of viper bite poisoning. Annals of Tropical Medicine and Parasitology, 1987, 81(2): 135-149.
[9] P. W. Coetzer, C. R. Tilbury. The epidemiology of snakebite in northern Natal. South African Medical Journal, 1982, 62(7): 206-212.
[10] Y. Sawai, et al. An Epidemiological study of snake bite in the southest Asia. South African Medical Journal, 1972, 42(3): 283- 307.
[11] C. Pochanugool, H. Wildde, K. Bhanganada, et al. Venomous snakebite in Thailand. II: Clinical experience. Military Medicine, 1998, 163(5): 318-323.
[12] R. Blaylock. Epidemiology of snakebite in Eshowe, KwaZuluNatal, South Africa. Toxicon, 2004, 43(2): 159-166.
[13] F. McGain, L. Aaron, J. W. David, et al. Snakebite mortality at Port Moresby General Hospital, Papua New Guinea, 1992-2001. Medical Journal of Australia, 2004; 181(11-12): 687-691.
[14] M. Y. Justin, L. Mark, M. M. Lindsay, et al. Antivenom dosing in 35 patient with severe brown snake (Pseugonaja) envenoming in Western Australia over 10 years. Medical Journal of Australia, 2004, 181(11-12): 703-705.
[15] Behrman: Nelson Textbook of Pediatrics, 17th Edition, Saunder, An Imprint of Elsevier. Chapter 708—Envenomations, 2004.
[16] C. C. Snyder, R. P. Knowles. Snakebites, Guidelines for practical management. Postgraduate Medical, 1988, 83(6): 52-60, 65- 68, 71-75.
[17] H. M. Parrish. Incidence of treated snakebites in the United States. Public Health Reports, 1966, 81(3): 269-276.
[18] C. A. Johnson. Management of snakebite. American Family Physician, 1991, 44(1): 174-180.
[19] P. Consroe, N. B. Egen, F. E. Russell, et al. Comparison of a new ovine antigen binding fragment (Fab) antivenin for United States Crotalidae with the commercial antivenin for protection against venom-induced lethality in mice. American Journal of Tropical Medicine and Hygiene, 1995, 53(5): 507-510.
[20] G. Juckett. Snakebite. In: R. E. Rakel, Ed., Saunders manual of medical practice. Saunders, New York, 2000: 1525-1528.
[21] T. P. Kuo, C. S. Wu. Clinico-pathological studies o snakebites in Taiwan. Journal of the Formosan Medical Association, 1972, 71(7): 447-466.
[22] J. C. Chen, S. J. Liaw, M. J. Bullard, et al. Treatment of poisonous snakebites in northern Taiwan. Journal of the Formosan Medical Association, 2000, 99(2): 135-139.
[23] W. B. Liao, C. W. Lee, Y. S. Tsai, et al. Influential factors affecting prognosis of snakebite patients’ management: Kaohsiung Chang Cung Momorial hospital experience. Chang Cung Medical Journal, 2000, 23(10): 577-583.
[24] M. Ovadia. Isolation and characterization of three hemorrhagic factors from the venom of Vipera palaestinae. Toxicon, 1978, 16(5): 479-487.
[25] I. H. Tsai, Y. M. Wang, Y. H. Chen, T. S. Tsai and Mc. Tu. Venom phospholipase A2 of bamboo veper (Trimeresurus stejnegeri): Molecular characterization, geographic variations and evidence of multiple ancestries. Biochemical Journal, 2004, 377: 215-223.
[26] C. Ouyang, C. M. Teng. Fibrinogenolytic enzymes of Trimeresurus mucrosquamatus venom. Biochimica et Biophysica Acta, 1976, 420(2): 298-308.
[27] C. Ouyang, C. M. Teng. The action mechanism of the purified platelet aggregation principle of Trimeresurus mucrosquanatus venom. Thrombosis and Haemostasis, 1976, 41(3): 475-490.
[28] C. Ouyang, T. F. Huang. Platelet aggregation inhibitors from Agkistrodon acutus snake venom. Toxicon, 1986, 24(11-12): 1099-1106.
[29] R. H. Chen, Y. C. Chen. Isolation of an acidic phospholipase A2 from the venom of Agkistrodon acutus (five pace snake) and its effect on platelet aggregation. Toxicon, 1989, 27(6): 675-682.
[30] C. C. Chen, C. M. Yang, F. R. Hu and Y. C. Lee. Penetrating ocular injury caused by venomous snakebite. American Journal of Ophthalmology, 2005, 140(3): 544-546.
[31] C. Y. Lee. Elapid Neurotoxins and mode of action. Clinical Toxicology, 1970, 3(3): 457-472.
[32] M. K. Lai, C. Y. Wen and C. Y. Lee. Local lesions caused by cardiotoxin isolated from Formosan cobra venom. Journal of the Formosan Medical Association, 1972, 71(6): 328-332.
[33] D. Z. Hung, M. Y. Liau and S. Y. Lin-Shiau. The clinical significance of venom detection in patients of cobra snakebite. Toxicon, 2003, 41(4): 409-415.
[34] T. L. Kao, C. W. Juan. Tongue viability after snakebite-an unusual occupational hazard. American Journal of Emergency Medicine, 2007, 25(9): 1083.e5-1083.e7.
[35] C. W. Juan, F. S. Wu, W. H. Chang, C. N. Lee and C. C. Chou. A case of envenomation by Bungarus Multicinctus. Journal of Emergency and Intensive Care Medicine, 1999, 10(2): 109-113.
[36] S. Limthongdul, C. Pochanugool and K. Meemano. Respiratory failure and its non-antivenin treatment in 37 adult neurotoxin snake-bite patients. In: P. Gopalakrishnakone and C. K. Tan, Eds., Progress in Venom and Toxin Research. Singapoye: Faculty of Medicine, National University of Singapore, 1987: 52-59.
[37] D. Z. Hung, M. L. Wu, J. F. Deng and S. Y. Lin-Shiau. Russell’s viper snakebite in Taiwan: Differences from other Asian countries. Toxicon, 2002, 40(9): 1291-1298.
[38] T. S. Chou, T. J. Lin, M. C. Kuo, T. Mee-Sun, D. Z. Hung and J. L. Tsai. Eight cases of acute renal failure from Vipera russelli formosensis venom after administration of antivenom. Veterinary and Human Toxicology, 2002, 44(5): 278-282.
[39] D. Z. Hung, Y. J. Yu, C. L. Hsu and T. J. Lin. Antivenom treatment and renal dysfunction in Russell’s viper snakebite in Taiwan: A case series. Transactions of the Royal Society of Tropical Medicine and Hygiene, 2006, 100(5): 489-494.
[40] D. Z. Hung, M. L. Wu, J. F. Peng, D. Y. Yang and S. Y. Lin-Shiau. Multiple thrombotic occlusions of vessels after Russell’s Viper Envenoming. Pharmacology amd Toxicology, 2002, 91(3): 106-110.
[41] K. P. Chang, C. S. Lai and S. D. Lin. Management of poisonous snake bites in southern Taiwan. Kaohsiung Journal of Medical, 2007, 23(10): 511-518.
[42] C. M. Yu, W. C. Huang, K. Y. Tung, H. T. Hsiao and S. Y. Ou. Prognostic factors of local necrosis due to poisonous snakebite-a clinical reciew in Mackay Memorial Hospital. Journal of Plastic Surgical Association R.O.C. 2005, 14(1): 31-40.
[43] J. B. Lopoo, J. F. Bealer, P. C. Mantor and D. W. Tuggle. Treating the snakebitten child in North America: A study of pit viper bites. Journal of Pediatric Surgery, 1998, 33(11): 1593-1595.
[44] H. M. Parrish, J. C. Goldner and S. L. Silberg. Comparison between snakebites in children and adults. Pediatrics. 1965, 36(2): 251-256.
[45] R. A. Weber, R. R. White. Crotalidae envenomation in children. Annals of Plastic Annals of Plastic Surgery, 1993, 2: 142-145.
[46] C. F. Chen, T. J. Lin, W. C. Hsu and H. W. Yang. Appropriate antivenom doses for six types of envenomations caused by snakes in Taiwan. Journal of Venomous Animals and Toxins Including Tropical Diseases, 2009, 15(3): 479-490.