Hans Journal of Ophthalmology
Vol.2 No.3(2013), Article ID:12358,3 pages DOI:10.12677/HJO.2013.23005
Pediatric Acute Retinal Necrosis—A Case Report
Department of Ophthalmology, Kaohsiung Veterans General Hospital, Kaohsiung
Email: ctchuang@vghks.gov.tw
Received: Jun. 11th, 2013; revised: Aug. 10th, 2013; accepted: Aug. 18th, 2013
Copyright © 2013 Chiu-Tung Chuang et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT:
Purpose: To report an uncommon case of acute retinal necrosis in a 5-year-old girl. Methods: Case report. Results: A 5-year-old girl presented with redness, ocular pain and blurred vision present for few days on the right eye. The past medical history revealed herpetic encephalitis at the age of 1. On examination, visual acuity was 6/60 on the right and 6/6 on the left. Slit-lamp examination showed moderate anterior uveitis and vitritis in her right eye. Fundoscopy showed large areas of peripheral circumferential retinal necrosis. Under the diagnosis of acute retinal necrosis due to its typical fundus lesions, treatment with intravenous Acyclovir and topical steroid eyedrops were started immediately. Pediatric examination and laboratory testing, including immunologic tests, were normal. After 10 days, treatment was changed to oral Valaciclovir and Prednisolone. Topical treatment was tapered gradually. The response was well initially, with resolution of retinitis patches and improvement of visual acuity to 6/20 in 3 weeks. Oral steroids were gradually reduced, and original lesions completely disappeared in 4 weeks, leaving only retinal pigment epithelial change. Seven weeks later, vision dropped to counting finger on the right due to rhegmatogeous retinal detachment. Conclusion: We report an uncommon case of acute retinal necrosis in a 5-year-old girl. This patient responded well to systemic antiviral medication and steroid initially but developed rhegmatogeous retinal detachment 7 weeks later.
Keywords: Acute Retinal Necrosis; Polymerase Chain Reaction; Prophylactic Vitrectomy
幼儿急性视网膜坏死之病例报告
庄秋同,吴宗典,朱明嫈,许淑娟
高雄荣民总医院眼科部,高雄
Email: ctchuang@vghks.gov.tw
摘 要:
目的:报告一个5岁女童罹患急性视网膜坏死之少见病例。方法:病例报告。结果:一名5岁女童因多日前突发性右眼红痛及视力模糊而求诊,病患于1岁时曾有疱疹病毒性脑炎之病史。眼科理学检查发现右眼视力为0.1,左眼为1.0。裂隙灯检查发现右眼前房及玻璃体皆有中度炎症反应,视网膜周边则出现坏死性区域。由于其典型之眼底病灶,故诊断为急性视网膜坏死,并开始给予静脉注射Acyclovir及类固醇眼药水治疗。儿科检查和实验室测试,包括免疫测试,都是正常的。十天后改为口服Valaciclovir并加上口服类固醇治疗。药效初期反应良好,三星期后视网膜坏死区域已减少,患眼视力也进步至0.3;口服类固醇逐步减量,原先之病灶于4星期后皆已消失,仅留下视网膜色素层变化,但于治疗7星期后倂发裂孔性视网膜剥离。结论:我们报告一例急性视网膜坏死发生于5岁女童之少见病例,病患经全身性抗病毒药物合倂口服类固醇治疗后一度恢复良好,但于治疗7星期后倂发裂孔性视网膜剥离。
收稿日期:2013年7月11日;修回日期:2013年8月10日;录用日期:2013年8月18日
关键词:急性视网膜坏死;聚合酶连锁反应;预防性玻璃体切除
1. 引言
急性视网膜坏死(Acute retinal necrosis, ARN)最早是由日本学者Uruyama 于1971年所提出[1]。ARN的病征包含有周边视网膜的坏死、阻塞性血管炎、虹彩炎及玻璃体炎等[2]。这个疾病大部份发生在成人,儿童并不常见[3],故我们于此报告一例发生于5岁女童之少见病例。
2. 病例报告
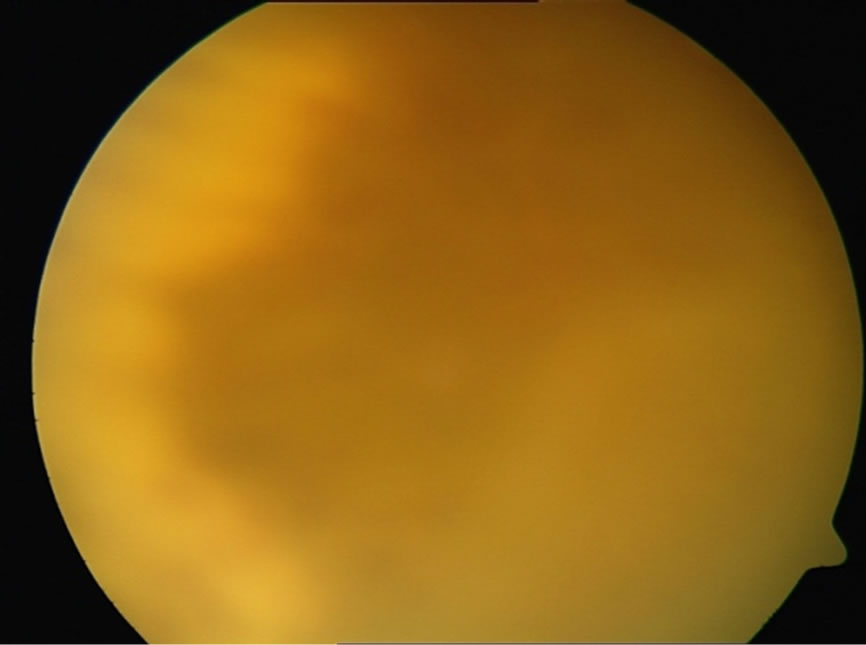
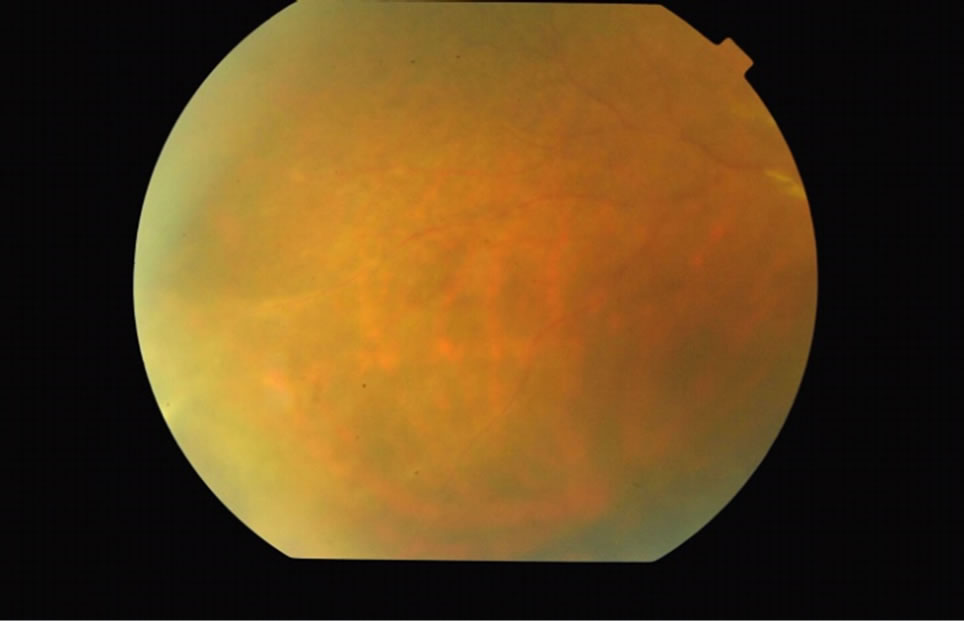
病患为一名5岁女童,因多日前突发性右眼红痛及视力模糊而求诊。病患于1岁时曾有疱疹病毒性脑炎之病史,但并无残留之后遗症。眼科理学检查发现右眼视力为0.1,左眼为1.0,双眼眼压正常。右眼前房及玻璃体皆有中度炎症反应,视网膜周边则出现黄白色坏死区域(图1)。小儿科会诊、血液常规、胸部X光、免疫学及感染性致病源之血清检查并无特别发现。由于其典型之眼底病灶,故诊断为急性视网膜坏死,并开始给予静脉注射抗病毒药物Acyclovir (200 mg每天3次)及类固醇眼药水1% Pred-Forte (每4小
 (a)
(a) (b)
(b)
Figure 1. Confluent peripheral retinal necrosis (a) temporal part (b) inferior part
图1. 视网膜周边出现黄白色坏死区域(a)颞侧(b)下方
时一次)治疗。十天后改为口服抗病毒药物Valaciclovir (400 mg每天3次)并加上口服类固醇Prednisolone (每天15 mg)治疗。经全身性抗病毒药物合倂口服类固醇治疗后,药效初期反应良好,三星期后视网膜坏死区域已减少,患眼视力也进步至0.3;之后口服类固醇逐步减量,原先之病灶于4星期后皆已消失,仅留下视网膜色素性变化(图2),但于治疗7星期后,病患视力突然急遽下降至眼前数指三十公分,经检查发现倂发裂孔性视网膜剥离(图3)。虽已帮病患安排玻璃体切除合并硅油填充手术,但病患并未回诊就医。
3. 讨论
ARN是由疱疹病毒家族的部份病毒所引起;其中水痘带状疱疹病毒(Varicella zoster virus, VZV)占大多数[4],单纯性疱疹第一型(Herpes simplex virus type 1, HSV-1)及第二型(HSV-2)次之,而巨细胞病毒(Cytomegalovirus, CMV)及伊波病毒(Epstein-Bar virus, EBV)则相当罕见。Ganatra曾报告由VZV及HSV-1引起的ARN患者通常年龄在25岁以上,而
 (a)
(a) (b)
(b)
Figure 2. Resolution of peripheral retinal necrosis after treatment for 4 weeks (a) temporal part (b) inferior part
图2. 原先之病灶于4星期后皆已消失,仅留下视网膜色素性变化 (a)颞侧(b)下方
 (a)
(a) (b)
(b)
Figure 3. Rhegmatogenous retinal detachment developed after treatment for 7 weeks (a) posterior part (b) inferior part
图3. 7星期后倂发裂孔性视网膜剥离(a)后极部(b)下方
HSV-2引起者则在25岁以下;若曾有中枢神经系统感染之病史,则单纯性疱疹病毒极可能为其致病原因[5]。本例患者过去曾有疱疹病毒性脑炎之病史,但可惜未做病毒学方面的检查,无法再次验证这一发现。
ARN的诊断主要是依据临床表征及病程,然而一些非典型表现之病患则需进一步检查,以免延误治疗。传统的病毒培养法既耗时又易有伪阴性,故聚合酶连锁反应(polymerase chain reaction, PCR)是最佳的检查工具;根据之前的研究报告,PCR的灵敏度可高达90%[5,6]。
ARN药物治疗的主要目的是尽快让患眼复原,同时避免对侧眼受到侵犯,由于大多数的ARN是VZV或HSV所引起,故静脉注射Acyclovir是治疗首选,建议剂量为静脉注射Acyclovir (5~10 mg/kg每天3次) 7至10天,之后改成口服Valaciclovir (1 g每天3次)1至3个月。然近来也有使用玻璃体内注射抗病毒药物作为辅助疗法[7,8],或仅使用口服Valaciclovir或Famciclovir成功治疗之报告[9,10]。全身性类固醇可以减少眼内发炎及恢复玻璃体清澈,但需于抗病毒药物开始使用后方可给予,初始剂量为每天每公斤1~2毫克,之后逐步减量,而局部类固醇眼药水则用于眼前段发炎之患者。有些学者亦建议使用抗凝血剂来减低血管阻塞的并发症[11],但并未有临床试验证实其效果。
视网膜剥离是ARN最严重的后遗症之一,也是造成视力丧失的主因,发生率可高达75%,有学者提出施以预防性雷射于病变处后缘,并指出可使视网膜剥离发生率有效降低[8,12];但亦有报告指出预防性雷射其实效果不佳[13],因其样本数通常太小,而适合接受雷射治疗者通常是玻璃体清澈病情较轻微者,故易有统计上的偏差[14]。近来有一些施行预防性玻璃体切除以避免视网膜剥离发生的报告[14,15],其作用主要是消除玻璃体对视网膜牵扯的力量,虽然于减少发生率部份确实让人振奋,但是最终视力却没有明显改善[14,16],或许视网膜剥离前已有视网膜缺血或视神经萎缩是可能之原因。本例患者因年纪小而无法配合预防性雷射之施行,于发生视网膜剥离后又未回诊接受手术治疗,故无法评估其视力预后,甚感可惜。我们之前曾有两例急性视网膜坏死发生视网膜剥离的成人病例,经玻璃体切除及硅油填充后视网膜皆复位良好,术后最佳矫正视力为0.1,或可作为视力预后之参考。
4. 结论
我们报告一例急性视网膜坏死发生于5岁女童之少见病例,病患经全身性抗病毒药物合倂口服类固醇治疗后一度恢复良好,但于治疗7星期后倂发裂孔性视网膜剥离。急性视网膜坏死病患发生视网膜剥离的机率甚高,目前预防视网膜剥离的预防性处置有二:一是于视网膜坏死处后缘做预防性雷射,另一则是施行预防性玻璃体切除;本例患者因年纪小而无法配合预防性雷射之施行,故若早期进行预防性玻璃体切除或许可以预防其视网膜剥离发生。
参考文献 (References)
[1] A. Uruyama, N. Yamada and T. Sasaki. Unilateral acute uveitis with periarteritis and detachment. Japanese Journal of Clinical Ophthalmology, 1971, 25: 607-619.
[2] G. N. Holland. Standard diagnostic criteria for the acute retinal necrosis syndrome. Executive Committee of the American Uveitis Society. American Journal of Ophthalmology, 1994, 117(5): 663-667.
[3] J. Tan, D. Byles, M. Stanforf, et al. Acute retinal necrosis in children caused by herpes simplex virus. Retina, 2001, 21(4): 344-347.
[4] W. W. Culbertson, M. S. Blumenkranz, J. S. Pepose, et al. Varicella-zoster virus is a cause of the acute retinal necrosis syndrome. Ophthalmology, 1986, 93(5): 559-569.
[5] J. B. Ganatra, D. Chandler, C. Santos, et al. Viral causes of acute retinal necrosis. American Journal of Ophthalmology, 2000, 129(2): 166-172.
[6] G. A. Short, T. P. Margolis, B. D. Kuppermann, et al. A polymerase chain reaction-based assay for diagnosing varicella-zoster virus retinitis in patients with acquired immunodeficiency syndrome. American Journal of Ophthalmology, 1997, 123(2): 157-164.
[7] K. K. Luu, I. U. Scott, N. A. Chaudhry, et al. Intravitreal antiviral injections as adjunctive therapy in the management of immunocompetent patients with necrotizing herpetic retinopathy. American Journal of Ophthalmology, 2000, 129(6): 811-813.
[8] B. Meghpara, G. Sulkowski, M. R. Kesen, et al. Long-term follow-up of acute retinal necrosis. Retina, 2010, 30(5): 795- 800.
[9] G. G. Emerson, J. R. Smith, D. J. Wilson, et al. Primary treatment of acute retinal necrosis with antiviral therapy. Ophthalmology, 2006, 113(12): 2259-2261.
[10] A. Aizman, M. W. Johnson and S. G. Elner. Treatment of acute retinal necrosis syndrome with oral antiviral medications. Ophthalmology, 2007, 114(2): 307-312.
[11] W. W. Culbertson, S. S. Atherton. Acute retinal necrosis and similar retinitis syndromes. International Ophthalmology Clinics, 1993, 33(1): 129-143.
[12] P. Sternberg, D. P. Han, J. H. Yeo, et al. Photocoagulation to prevent retinal detachment in acute retinal necrosis. Ophthalmology, 1988, 95(10): 1389-1393.
[13] H. R. McDonald, H. Lewis, A. E. Kreiger, et al. Surgical management of retinal detachment associated with the acute retinal necrosis syndrome. British Journal of Ophthalmology, 1991, 75(8): 455-458.
[14] J. Hillenkamp, B. Nölle, C. Bruns, et al. Acute retinal necrosis: Clinical features, early vitrectomy, and outcomes. Ophthalmology, 2009, 116(10): 1971-1975.
[15] T. Ishida, S. Sugita, et al. Prophylactic vitrectomy for acute retinal necrosis. Japanese Journal of Ophthalmology, 2009, 53(5): 486-489
[16] Y. Usui, M. Takeuchi, Y. Yamauchi, et al. Pars plana vitrectomy in patients with acute retinal necrosis syndrome: Surgical results in 52 patients. Nippon Ganka Gakkai Zasshi, 2010, 114(4): 362- 368.