Advances in Clinical Medicine
Vol.
13
No.
08
(
2023
), Article ID:
70987
,
8
pages
10.12677/ACM.2023.1381871
CD19/CD3双抗治疗儿童B-ALL合并特鲁索综合征1例并文献复习
胡晓晶,张磊,徐以凤,梁卉*
青岛大学附属妇女儿童医院血液肿瘤科,山东 青岛
收稿日期:2023年7月23日;录用日期:2023年8月15日;发布日期:2023年8月22日

摘要
目的:探索应用CD19/CD3双抗治疗儿童B型急性淋巴细胞白血病(B-Acute Lymphoblastic Leukemia, B-ALL)合并特鲁索综合征,为此类患儿寻求更佳治疗手段。方法:回顾性分析1例B-ALL合并特鲁索综合征患儿的诊疗过程,并结合文献进行复习。结果:患儿,男,7岁,因“发热、血象异常”就诊,经形态学(M)、免疫学(I)、细胞遗传学(C)和分子生物学(M),即MICM综合分型确诊为B-ALL。在诱导治疗期间微小残留(MRD)未转阴,继发特鲁索综合征,患儿短时间内无法进行强化及巩固化疗、形态学复发风险升高,而CD19/CD3双抗相对于传统强化疗,其骨髓抑制轻,不良反应少,为患儿长期缓解争取了时间。结论:对于常规化疗效果不佳或不能耐受化疗的B-ALL患儿,CD19/CD3双抗治疗可作为有效的过度治疗方案,可以为此类患儿提供新的治疗选择。
关键词
B型急性淋巴细胞白血病,儿童,特鲁索综合征,CD19/CD3双抗

CD19/CD3 Dual Antibody Treatment of Children B-ALL Combined with Trousseau Syndrome: A Case Report and Literature Review
Xiaojing Hu, Lei Zhang, Yifeng Xu, Hui Liang*
Department of Hematology and Oncology, Women and Children’s Hospital of Qingdao University, Qingdao Shandong
Received: Jul. 23rd, 2023; accepted: Aug. 15th, 2023; published: Aug. 22nd, 2023

ABSTRACT
Objective: This study aimed to explore the application of CD19/CD3 dual antibody in the treatment of children with B-Acute Lymphoblastic Leukemia (B-ALL) complicated with Trousseau syndrome, and to seek better treatment for these children. Methods: The treatment of a child with B-ALL combined with Trousseau’s syndrome was retrospectively analyzed and reviewed in light of the literature. Results: The patient, a male, 7 years old, was diagnosed with B-ALL due to “fever and abnormal hematology” and was diagnosed as B-ALL by Morphology (M), Immunology (I), Cytogenetics (C), and Molecular biology (M), namely MICM comprehensive typing. During induction therapy, the patient was combined with Trousseau’s syndrome, and children could not receive chemotherapy such as reinforcement and consolidation within a short time, resulting in an increased risk of morphological recurrence. However, the application of CD19/CD3 dual antibody provided a distinct advantage of effectively eliminating microscopic residuals (MRD) and reducing the incidence of complications caused by chemotherapy drugs in patients. This allowed for additional time to achieve long-term remission in the child. Conclusion: CD19/CD3 dual antibody therapy can be used as an effective overtreatment for B-ALL children with poor conventional chemotherapy or who cannot tolerate chemotherapy and can provide a new treatment option for such children.
Keywords:B-Acute Lymphoblastic Leukemia, Children, Trousseau Syndrome, CD19/CD3 Dual Antibody

Copyright © 2023 by author(s) and Hans Publishers Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY 4.0).
http://creativecommons.org/licenses/by/4.0/


1. 引言
B-ALL是儿童最常见的恶性肿瘤 [1] ,虽然大多数患有B-ALL的儿童通过现代风险分层化疗方案可以达到临床治愈,五年总生存率达到80%~90% [2] ,但由于其临床病程多变,包括病情特点,患者个体差异、分子遗传学异常和治疗反应等,其治疗失败仍然是一部分患儿在诊断后5年内死亡的主要原因 [3] ,需要寻找新的治疗方法以改善治疗结局。目前,国内将CD19/CD3双抗联合化疗用于治疗儿童B-ALL的经验较少,本研究报道1例诱导治疗期合并特鲁索综合征的B-ALL患儿,应用CD19/CD3双抗治疗后效果良好,桥接后续化疗过程顺利,以此进行文献复习,希望为常规化疗效果不佳或者是化疗不耐受的B-ALL患儿提供新的诊疗思路。
2. 临床资料
患儿,男,7岁,2022.06.11因“发热3天,发现血象异常2天”入院。院外测体温最高39℃,无寒战、抽搐,热峰4~5次/日,无咳喘,发热时伴头痛,前额为主,无腹痛、吐泻等不适,口服“感冒药”治疗效欠佳。查体:神志清,反应一般,皮肤黏膜苍黄,双颈部扪及数个淋巴结,最大3 cm × 2 cm,质地韧,无触痛,口唇略苍白,胸骨无压痛,腹软,腹部未触及包块,肝右肋下5 cm,脾左肋下3 cm,均质韧。辅助检查:血常规:白细胞计数(White Blood Cell count, WBC) 3.65 × 109/L,红细胞计数(Red Blood Cell count, RBC) 2.19 × 1012/L,血红蛋白(Hemoglobin, Hb) 6 g/L,血小板计数(Platelet count, PLT) 99 × 109/L,中性粒细胞绝对值(Neutrophil, NEU) 1.03 × 109/L,C-反应蛋白(C-reactive Protein, CRP) 76.56 mg/L,以“发热、血象异常原因:急性白血病?”收住院。
入院后进一步完善实验室检查:血生化、凝血功能未见异常,异常白细胞示幼稚细胞占5%,骨髓涂片提示原幼淋巴细胞占89%,形态学考虑ALL,外送骨髓免疫分型可见异常原始B淋巴细胞,异常细胞群占有核细胞86.86%,表达CD34、CD38、HLA-DR、CD19、CD79a、TDT等,部分表达CD13、CD10,不表达CD117、CD20、MPO、cCD3、cIgM、sIgM及其他髓系、淋系标志;骨髓FISH示MLL基因重排、BCR-ABL及TEL/AML、MYC融合基因均阴性;白血病43种融合基因示阴性;染色体示可见克隆性异常,del (3p),de1 (6q),t(12:12)-17,+add(22p)。血液系统疾病基因突变筛查:与疾病密切相关及可能相关的突变位点均未检测出,其他突变位点:FAT1、FDGFRB、HI3、RB1。头颅MRI检查符合白血病骨改变,脑实质未见异常。心电图、生殖系统超声未见异常。经MICM综合分型诊断为急性B淋巴细胞白血病。
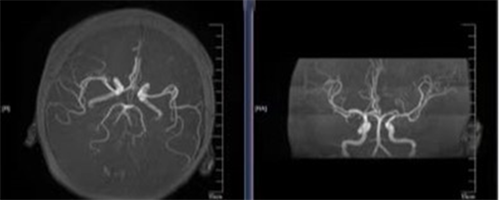
Figure 1. 2022.07.17 MRA showed no abnormalities
图1. 2022.07.17 MRA无异常
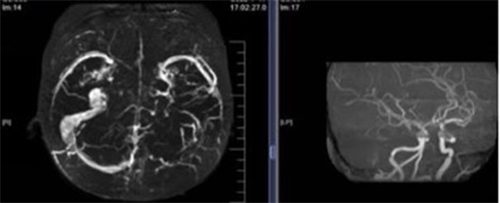
Figure 2. 2022.07.17 MRV: 1. The left transverse sinus and superior sagittal sinus were filled with defects, and occlusion was considered. 2. Intermittent imaging of left sigmoid sinus
图2. 2022.07.17 MRV:1. 左侧横窦、上矢状窦充盈缺损,考虑闭塞;2. 左侧乙状窦断续显影
治疗过程:评估无化疗禁忌,按化疗方案给予VDLD (长春地辛2.85 mg × 2次、柔红霉素28.5 mg × 2次、培门冬酶2375 U × 1次、地塞米松)方案化疗,期间行腰椎穿刺 + 鞘内注射化疗药物术2次,脑脊液检查无异常。化疗19天(2022.06.30)复查骨髓细胞学示原始幼稚淋巴细胞占23%,MRD 28.7%,提示未缓解,遂入高危组给予(长春地辛3 mg × 2次、伊达比星9 mg × 1次、多柔比星脂质体20 mg × 1次、培门冬酶2500 U × 1次、强的松)方案化疗,于第35天(2022.07.16)复查骨髓细胞学示形态学转阴,MRD 0.63%,可继续化疗。但随后患儿开始出现头痛、右上肢体抖动等情况,症状多为活动时出现,查体示血压正常,四肢肌力、肌张力正常,完善凝血常规、血栓弹力图检测示血小板性低凝,纤维蛋白原性低凝,头颅MRA (见图1)未见明显异常,MRV (见图2)提示静脉窦血栓,治疗上应用低分子肝素钙抗凝、口服维生素B12营养神经及卧床休息等对症支持处理,治疗后患儿症状缓解,但其后仍间断出现头痛及右侧肢体活动、感觉异常等不适,复查MRI (见图3)考虑特鲁索综合征可能性大;MRV (见图4)考虑静脉栓塞改变,遂继续予低分子肝素钙治疗。在患儿头痛症状缓解、无活动性出血情况发生后,考虑患儿短时间内进行后续强化及巩固化疗难度大,决定于梗塞相对稳定后立即启动免疫治疗,经家长知情同意并表示积极配合治疗后,于08.04始予贝林妥欧单抗(0.47 mL/日d1~d6,1.5 mL/日d7~d28)治疗,疗程共计28天,应用贝林妥欧单抗治疗期间患儿的头痛、头晕症状改善,监测血压、计出入比维持在正常范围,定期监测血常规(见图5)、凝血常规(见图6)、生化未见明显异常,应用该药物过程顺利,患儿一般情况良好,未再诉不适。患儿在应用贝林妥欧单抗后持续予皮下注射低分子肝素钙治疗,于2022.09.01复查骨髓形态学示完全缓解,MRD转阴,复查头颅MRV及MRI (见图7)提示脑梗塞明显好转。随访至2023年6月,该患儿已确诊白血病11.5月余,目前处于脑梗塞恢复期,应用贝林妥欧单抗后桥接后续化疗过程均顺利,末次入院行HR-2’方案(地塞米松 + 甲氨蝶呤 + 长春地辛 + 异环磷酰胺 + 蒽环类药物 + 培门冬酶)化疗,现顺利进行中,后续将继续化疗后桥接造血干细胞移植(Hematopoietic Stem Cell Transplantation, HSCT)。
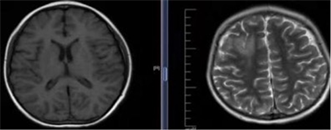
Figure 3. 2022.07.23 MRI: Abnormal signals were found in bilateral frontal and right parietal lobes and superior sagittal sinus: multiple venous cerebral infarction, considering Trousseau’s syndrome
图3. 2022.07.23 MRI:双侧额叶及右侧顶叶异常信号及上矢状窦异常信号——多发静脉性脑梗塞,考虑特鲁索综合征

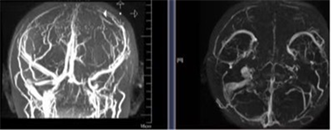
Figure 4. 2022.07.23 MRV: Multiple abnormal changes were occurred in bilateral transversal sinus, left sigmoid sinus, sinuses, and superior sagittal sinus: venous embolization was considered
图4. 2022.07.23 MRV:双侧横窦、左侧乙状窦、窦汇及上矢状窦多发异常改变——考虑静脉栓塞改变
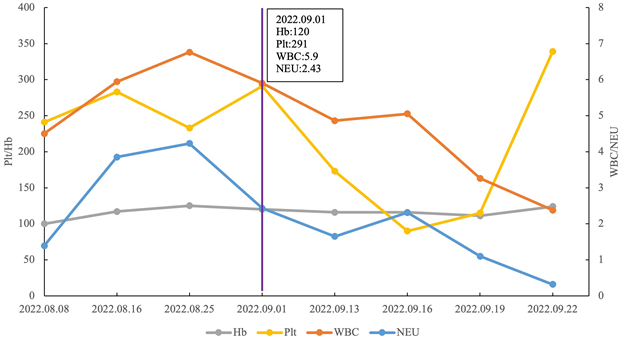
Figure 5. Hemogram changes of children treated with blinatumomab
图5. 贝林妥欧单抗治疗期间患儿血象变化情况
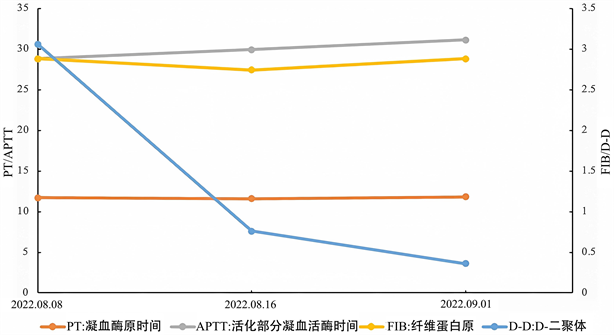
Figure 6. Changes of blood coagulation routine in children treated with blinatumomab
图6. 贝林妥欧单抗治疗期间患儿凝血常规变化情况
 (a)
(a)
 (b)
(b)
Figure 7. 2022.09.02 MRI and MRV: Multiple venous embolization in the left transverse sinus, sigmoid sinus and superior sagittal sinus changed during the recovery period. Embolization in the right transverse sinus and sinuses was less obvious than before, and slightly coarse collateral venous reflux was observed around the left sigmoid sinus
图7. 2022.09.02 MRI、MRV:左侧横窦、乙状窦及上矢状窦多发静脉栓塞恢复期改变,右侧横窦、窦汇部栓塞较前已不明显,左侧乙状窦周见略粗大静脉侧枝回流
3. 讨论
血液恶性肿瘤是最常见的儿童癌症类型,B-ALL是儿童中最常见的血液系统恶性肿瘤之一,约占所有儿童ALL病例的85% [4] 。目前国内患者的治疗以化疗为主,但对于化疗不耐受进而导致治疗失败的患者,效果仍不够理想,亟需更有效的治疗方法改变此类患者的生存现状。目前,免疫治疗已成为近年来治疗B-ALL的热点,贝林妥欧单抗作为一种双特异性免疫抗体药物也逐渐进入人们的视野 [5] [6] ,但贝林妥欧单抗联合常规化疗治疗儿童B-ALL安全性如何,能否进一步提高常规化疗后出现并发症的患儿的治疗效果,目前尚缺乏更多临床资料。
贝林妥欧单抗是一种双特异性T细胞接合抗体 [7] ,连接针对CD19和CD3的两种抗体的靶向区域 [8] [9] ,其中CD19由前体B-ALL细胞表达,CD3是T细胞受体(T Cell Receptor, TCR)复合物的恒定部分,介导T细胞受体信号传导 [10] 。贝林妥欧单抗将TCR复合物上的CD3与良性或恶性B细胞上的CD19连接,在密切接触区形成细胞溶解突触 [8] ,进而导致CD19阳性的细胞溶解,用于治疗复发/难治性急性淋巴细胞白血病(R-R ALL) [11] 。目前在R-R ALL中使用贝林妥欧单抗已显示出良好的效果,特别是作为造血干细胞移植的桥接工具 [12] 。国外一项回顾性研究 [13] 评估了13例1~18岁的儿童R/R BCP-ALL患者接受贝林妥欧单抗单药治疗的疗效,其中接受倍利妥治疗的患者总缓解率为85% (11/13),13例儿童患者中有11例后续可行HSCT治疗。对这些患者进行随访,中位随访时间为25.4个月,贝林妥欧单抗治疗应答者的总生存期为100%,而缺乏应答的患者预后不佳(2例均死亡)。迄今为止,11例接受贝林妥欧单抗治疗的患者在HSCT后仍然存活,处于持续缓解状态且最小残留病变流式细胞术的检测结果呈阴性,说明贝林妥欧单抗桥接HSCT后效果良好。国外研究显示,贝林妥欧单抗治疗复发B-ALL的MRD转阴率达75%,其中,Brown等 [14] 的研究报道显示了对B-ALL首次复发的儿童、青少年和年轻人,诱导后巩固贝林妥欧单抗与化疗对无病生存的影响,其中位随访时间为2.9年,贝林妥欧单抗组2年无病生存率为54.4%,化疗组为39.0% (疾病进展或死亡率的风险比为0.70 [95% CI, 0.47~1.03];单侧P = 0.03),贝林妥欧单抗组的两年总生存率为71.3%,化疗组为58.4% (死亡率风险比为0.62 [95% CI, 0.39~0.98];单侧P = 0.02)。综上所述,贝林妥欧单抗能显著延长该类患儿的无病生存期和总生存期,且安全性和耐受性良好 [12] [14] [15] 。
在2022年,贝林妥欧单抗治疗中国儿童R/R B-ALL的适应症已获批 [16] ,对于R-R ALL患者,越早使用贝林妥欧单抗获益越多,推荐首次复发者的挽救治疗和早期复发、诱导后MRD阳性即中高危患者的巩固治疗,后续桥接HSCT将获得更长期的生存。该例患儿于08.03查颅脑CT示多发静脉性脑梗塞恢复期改变,较前范围减小,提示脑梗塞、脑出血趋于平稳,进入恢复期。但对于患儿的后续治疗,是选择继续化疗,还是免疫治疗引起了医生的思考。首先,化疗中的某些药物,比如培门冬酶会影响到患儿的凝血功能,可能再次导致血栓形成,严重的血栓形成使该药物的应用受限;其次,患儿诱导缓解期间发生严重脑梗,后续化疗时患儿的耐受性降低,形态学复发风险高,需警惕肿瘤原发耐药可能。此外,患儿基因突变筛查全套检查中FAT1基因检测到p.V1373I突变,人群数据库显示此突变在人群中的比例小于1%,功能性预测此突变可能影响蛋白功能,目前临床意义未明,主要见于ALL和慢性淋巴细胞白血病(CLL),其在成人B-ALL中的突变率约为10%,在儿童B细胞急性淋巴细胞白血病中,FAT1基因过表达提示疾病的复发风险增高。患儿基础情况不佳,基因检查提示复发风险升高,因此后续化疗进展困难、治疗难度增大。虽然与儿童传统化疗相比,贝林妥欧单抗改变了B-ALL患儿的治疗模式,具有更高的MRD阴性反应率和更低的毒性方面的优势 [8] ,在一定比例的患者中诱导了深度缓解,但是,国内将贝林妥欧单抗用于治疗儿童B-ALL的经验仍然较少。Elitzur等 [17] 报道了报告了11例儿童B-ALL患者,在不能耐受化疗严重不良反应后接受贝林妥欧单抗治疗,所有患者均恢复并成功桥接进一步的抗白血病治疗。国内游红亮等人 [18] 关于“贝林妥欧单抗治疗儿童急性B淋巴细胞白血病10例临床分析”研究中有1例患儿在合并严重念珠菌感染时应用贝林妥欧单抗而后继续化疗,随访结束时此患儿未复发,效果良好。而该例患儿诱导治疗期间合并神经系统并发症,应用贝林妥欧单抗治疗后具有良好的疗效及安全性,桥接后续化疗过程顺利,为后续长期缓解争取了时间。提示贝林妥欧单抗可作为有效的过度治疗方案,为常规化疗效果不佳或不能耐受化疗的B-ALL患儿提供新的治疗选择。
研究显示 [19] ,目前应用贝林妥欧单抗治疗下的观察到的主要不良事件包括细胞因子释放综合征(Cytokine Release Syndrome, CRS)和神经毒性 [20] [21] ,这两种情况在大多数情况下都很容易控制。细胞因子释放综合征通常表现为各种轻微症状,如发烧、疲劳、头痛、关节痛、肌痛或皮疹;不受控制的全身炎症可能发展到危及生命的情况,表现为低血压、呼吸系统疾病、弥漫性血管内凝血和毛细血管渗漏、噬血细胞性淋巴组织细胞增多症和多器官系统衰竭。Kiyoi等 [22] 关于贝林妥欧单抗在日本成人R-R ALL的1b/2期研究中报道了CRS和神经系统事件,该药物相关的CRS发生在几名患者中,其中1名患者因被认为与贝林妥欧单抗治疗相关的4级CRS而停止研究,此外,1例患者出现3级吞咽下神经事件。而该报道中唯一致命的不良事件,肿瘤溶解综合征,是由于疾病进展,与贝林妥欧单抗治疗无关。该例患儿在应用贝林妥欧过程中没有发生严重的不良反应,没有危及生命的情况发生,仅表现了一些轻微症状,即发热伴肢体疼痛,给予“布洛芬”治疗后症状缓解,符合应用该药物后表现出来的轻微症状,应用该药物后安全性及耐受性良好,与文献报道相符。
4. 结论
综上,本病例应用贝林妥欧单抗后桥接化疗效果良好,由于患儿随访时间短,个案的成功不足以证明CD19/CD3双抗桥接后续化疗会彻底改善此类患儿的结局,未来我们仍需要更多的研究去探讨其最佳剂量、疗程及联合化疗方案,希望大样本的研究为此类B-ALL儿童带来治愈机会。
文章引用
胡晓晶,张 磊,徐以凤,梁 卉. CD19/CD3双抗治疗儿童B-ALL合并特鲁索综合征1例并文献复习
CD19/CD3 Dual Antibody Treatment of Chil-dren B-ALL Combined with Trousseau Syn-drome: A Case Report and Literature Review[J]. 临床医学进展, 2023, 13(08): 13388-13395. https://doi.org/10.12677/ACM.2023.1381871
参考文献
- 1. Contreras, C.F., Higham, C.S., Behnert, A., et al. (2021) Clinical Utilization of Blinatumomab and Inotuzumab Immunotherapy in Children with Relapsed or Refractory B-Acute Lympho-blastic Leukemia. Pediatric Blood & Cancer, 68, e28718. https://doi.org/10.1002/pbc.28718
- 2. Fabrizio, V.A., Phillips, C.L., Lane, A., et al. (2022) Tisagenlecleucel Outcomes in Relapsed/Refractory Extramedullary ALL: A Pediat-ric Real World CAR Consortium Report. Blood Advances, 6, 600-610. https://doi.org/10.1182/bloodadvances.2021005564
- 3. Hoffman, L.M. and Gore, L. (2014) Blinatumomab, a Bi-Specific Anti-CD19/CD3 BiTE® Antibody for the Treatment of Acute Lymphoblastic Leukemia: Perspectives and Current Pediatric Applications. Frontiers in Oncology, 4, Article 63. https://doi.org/10.3389/fonc.2014.00063
- 4. Queudeville, M. and Ebinger, M. (2021) Blinatumomab in Pediatric Acute Lymphoblastic Leukemia—From Salvage to First Line Therapy (A Systematic Review). Journal of Clinical Medi-cine, 10, Article 2544. https://doi.org/10.3390/jcm10122544
- 5. Topp, M.S., Zimmerman, Z., Cannell, P., et al. (2018) Health-Related Quality of Life in Adults with Relapsed/Refractory Acute Lymphoblastic Leukemia Treated with Blinatumomab. Blood, 131, 2906-2914. https://doi.org/10.1182/blood-2017-09-804658
- 6. Brischwein, K., Schlereth, B., Guller, B., et al. (2006) MT110: A Novel Bispecific Single-Chain Antibody Construct with High Efficacy in Eradicating Established Tumors. Molecular Immunology, 43, 1129-1143. https://doi.org/10.1016/j.molimm.2005.07.034
- 7. 解姣, 杜薇薇, 刘素香, 等. 贝林妥欧单抗治疗儿童复发急性B淋巴细胞白血病3例临床分析[J]. 中国小儿血液与肿瘤杂志, 2022, 27(6): 379-382.
- 8. Duffy, C., Santana, V., Inaba, H., et al. (2022) Evaluating Blinatumomab Implementation in Low- and Middle-Income Countries: A Study Protocol. Implementation Science Communications, 3, Article No. 62. https://doi.org/10.1186/s43058-022-00310-5
- 9. Pawinska-Wasikowska, K., Wieczorek, A., Balwierz, W., et al. (2022) Blinatumomab as a Bridge Therapy for Hematopoietic Stem Cell Transplantation in Pediatric Refractory/Relapsed Acute Lymphoblastic Leukemia. Cancers, 14, Article 458. https://doi.org/10.3390/cancers14020458
- 10. Brown, P.A., Ji, L., Xu, X., et al. (2021) Effect of Postreinduction Therapy Consolidation with Blinatumomab vs Chemotherapy on Disease-Free Survival in Children, Adolescents, and Young Adults with First Relapse of B-Cell Acute Lymphoblastic Leukemia: A Randomized Clinical Trial. Journal of the American Medical Association, 325, 833-842. https://doi.org/10.1001/jama.2021.0669
- 11. Nguyen, K., Devidas, M., Cheng, S.C., et al. (2008) Factors Influ-encing Survival after Relapse from Acute Lymphoblastic Leukemia: A Children’s Oncology Group Study. Leukemia, 22, 2142-2150. https://doi.org/10.1038/leu.2008.251
- 12. Chinese Medical Association (2022) Chinese Consensus for the Bispeific T Cell Engager in the Treatment of B-Cell Acute Lymphoblastic Leukemia (2022). Chinese Journal of He-matology, 43, 448-455.
- 13. Elitzur, S., Arad-Cohen, N., Barzilai-Birenboim, S., et al. (2019) Blinatumomab as a Bridge to Further Therapy in Cases of Overwhelming Toxicity in Pediatric B-Cell Precursor Acute Lymphoblastic Leukemia: Report from the Israeli Study Group of Childhood Leukemia. Pediatric Blood & Cancer, 66, e27898. https://doi.org/10.1002/pbc.27898
- 14. 游红亮, 李远方, 路娜丹, 等. 贝林妥欧单抗治疗儿童急性B淋巴细胞白血病10例临床分析[J]. 中华实用儿科临床杂志, 2023, 38(7): 538-541.
- 15. Chitadze, G., Laqua, A., Lettau, M., Baldus, C.D. and Brüggemann, M. (2020) Bispecific Antibodies in Acute Lymphoblastic Leukemia Therapy. Expert Re-view of Hematology, 13, 1211-1233. https://doi.org/10.1080/17474086.2020.1831380
- 16. Liu, D.L., Zhao, J.J., Song, Y.P., Luo, X.F. and Yang, T. (2019) Clinical Trial Update on Bispecific Antibodies, Antibody-Drug Conjugates, and Antibody-Containing Regimens for Acute Lymphoblastic Leukemia. Journal of Hematology & Oncology, 12, Article No. 15. https://doi.org/10.1186/s13045-019-0703-z
- 17. Sigmund, A.M., Sahasrabudhe, K.D. and Bhatnagar, B. (2020) Evaluating Blinatumomab for the Treatment of Relapsed/Refractory All: Design, Development, and Place in Therapy. Blood and Lymphatic Cancer: Targets and Therapy, 10, 7-20. https://doi.org/10.2147/BLCTT.S223894
- 18. Jiang, M., Guo, X., Yuan, L., et al. (2020) Killer Cell Immunoglobulin-Like Receptor Gene Cluster Predisposes to Sus-ceptibility to B-Cell Acute Lymphoblastic Leukemia in Chinese Children. International Journal of Clinical and Experi-mental Pathology, 13, 536-542.
- 19. Rabilloud, T., Potier, D., Pankaew, S., et al. (2021) Single-Cell Profiling Identifies Pre-Existing CD19-Negative Subclones in a B-ALL Patient with CD19-Negative Relapse after CAR-T Therapy. Nature Communications, 12, Article No. 865. https://doi.org/10.1038/s41467-021-21168-6
- 20. Alsagaby, S.A. (2019) Omics-Based Insights into Therapy Failure of Pediatric B-Lineage Acutes Lymphoblastic Leukemia. Oncology Reviews, 13, 149-155. https://doi.org/10.4081/oncol.2019.435
- 21. Goroshchuk, O., Vidarsdottir, L., Björklund, A.C., et al. (2020) Targeting Plk1 with siRNNs in Primary Cells from Pediatric B-Cell Acute Lymphoblastic Leukemia Patients. Scientific Reports, 10, Article No. 2688. https://doi.org/10.1038/s41598-020-59653-5
- 22. Kiyoi, H., Morris, J.D., Oh, I., et al. (2020) Phase 1b/2 Study of Blinatumomab in Japanese Adults with Relapsed/Refractory Acute Lymphoblastic Leukemia. Cancer Science, 111, 1314-1323. https://doi.org/10.1111/cas.14322
NOTES
*通讯作者。