Hans Journal of Surgery
Vol.07 No.02(2018), Article ID:24424,6
pages
10.12677/HJS.2018.72010
A Case of Merkel Cell Carcinoma and the Review of Literature
Mingjian Wang, Siyuan Li, Peng Zhao, Qinghai Meng, Huizhong Lin*
Department of Genteral Surgery, Qingdao Municipal Hospital, Qingdao Shandong

Received: Mar. 28th, 2018; accepted: Apr. 12th, 2018; published: Apr. 19th, 2018

ABSTRACT
Merkel cell carcinoma (MCC) is a rare neuroendocrine, cutaneous malignancy that is highly aggressive. MCC tumourigenesis is linked to the presence of clonally integrated Merkel cell polyomavirus (MCPyV) and mutagenesis from ultraviolet (UV) light exposure. MCC presents as a firm, painless, rapidly enlarging, red-violet cutaneous tumour nodule that is typically dome-shaped. The diagnosis of MCC mainly relies on clinical manifestations, immunohistochemistry, histopathology and electron microscopy. The treatment of MCC is based on surgery plus chemotherapy and radiotherapy. MCC is an aggressive malignancy with frequent recurrences and a high mortality rate. MCC is easily missed and misdiagnosed.
Keywords:Merkel Cell Carcinoma, Diagnosis, Treatment, Prognosis
Merkel细胞癌1例并文献回顾
王明建,李思源,赵鹏,孟庆海,林惠忠*
青岛大学附属青岛市市立医院,普外科,山东 青岛

收稿日期:2018年3月28日;录用日期:2018年4月12日;发布日期:2018年4月19日

摘 要
Merkel细胞癌(MCC)是一种罕见的原发于皮肤的恶性神经内分泌肿瘤,具有高度侵袭性。其发病原因主要与紫外线直接照射以及Merkel细胞多瘤病毒感染相关。以质硬、无痛以及迅速增大的紫红色圆顶状肿瘤结节为其主要临床表现。目前MCC的诊断主要依靠临床表现、免疫组化、病理组织学及电镜检查。其主要治疗方案为:手术加放化疗。MCC侵袭性强,具有高复发率及死亡率,易误诊及漏诊。
关键词 :Merkel细胞癌,诊断,治疗,预后

Copyright © 2018 by authors and Hans Publishers Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/


1. 引言
麦克尔细胞癌(Merkel cell carcinoma, MCC)是一种神经内分泌癌,原发于皮肤,由Toker [1] [2] 于1972年首次报道。MCC恶性程度较高,严重威胁患者的生命。目前在国内发病较少,误诊率及漏诊率较高。本文就本院收治的一位Merkel细胞癌病例进行分析探讨。旨在加深临床对本病的认识,以提高诊治水平。
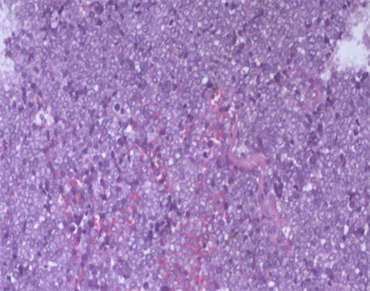
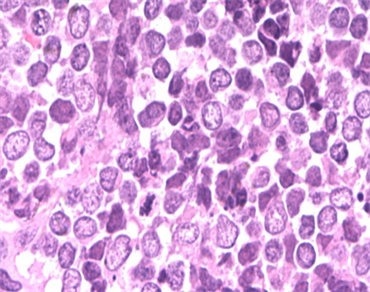
病情简介:患者,女性,75岁。发现右前臂肿物4月余,加速生长1月。于2016-5-17日来我院就诊。专科查体:右前臂桡测肘关节窝下5 cm,皮下肿块,大小约3 × 4 cm,周围边界欠清楚,表面不光滑,皮肤局部充血,活动度差。完善相关辅助检查:B超示:右前臂内侧皮下软组织内见混合回声团,大小约2.8 × 1.9 × 4.0 cm,边界尚清,形态尚规则,内回声团不均,见斑片强状回声,CDFI示:内见较丰富血流信号。考虑炎性包块可能。肿瘤标记物及其他相关检查未见明显异常。于2016-05-19日行右前臂皮肤肿物扩大切除术。术中见右前臂实行肿物,大小约4.0 × 3.0 cm,活动度差,向皮下浸润性生长,距肿瘤边缘2 cm行肿瘤完整切除。术中快速冰冻病理诊断示:皮肤恶性肿瘤,考虑麦克尔细胞癌。术后石蜡结果证实为麦克尔细胞癌。术后病理表现如图1、图2,相关免疫组织化学表现如图3~图5。
该患者免疫组化结果为:TTF-1(-),CK-7(-)CK20(+)Ki-67(90%)CK(+)Syn(+)CgA(+)CD56(+)。病理诊断结果:Merkel细胞癌。患者术后未行放化疗,半年后在原发部位复发。
 (a)
(a) 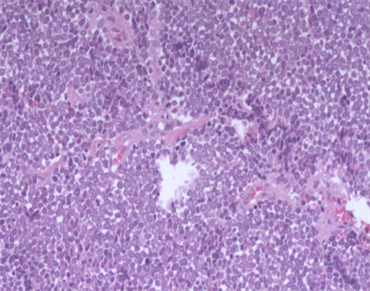 (b)
(b)
Figure 1. Merkel cell carcinoma histopathology HE staining (10 × 10)
图1. Merkel细胞癌组织病理HE染色(10 × 10)
 (a)
(a)  (b)
(b)
Figure 2. Merkel cell carcinoma histopathology HE staining (10 × 40)
图2. Merkel细胞癌组织病理HE染色(10 × 40)

Figure 3. Immunochemistry CD56(+)
图3. 免疫组化:CD56(+)

Figure 4. Immunochemistry: CgA(+)
图4. 免疫组化:CgA(+)
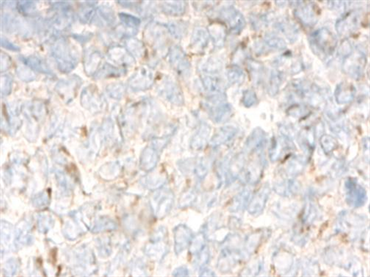
Figure 5. Immunochemistry: CK(+)
图5. 免疫组化:CK(+)
2. 流行病学及发病机
MCC的发病率极低,且在世界不同范围内发病率存在差异性。据欧洲罕见癌症监测(RARECARE)数据库报道:欧洲1995年至2002年间,发病率为0.13/100,000 [3] 。而美国国立癌症研究所(SEER)于2011年在美国的调查数据分析:发病率为0.79/100,000 [4] 。澳大利亚的MCC发病率最高,根据对1993年至2010年间的数据分析:其发病率为1.6/100,000 [5] 。与上述组织调查相比,中国的发病率更低,仅为个案报道。MCC的发病机制目前还尚未明确。有些观点认为其可能与Merkel细胞多瘤病毒(MCV或MCPyV,为SV40病毒的亚型)的感染有关。后续的研究也发现MCC患者体内MCV感染的检出率为43%~96% [6] 。另一种观点认为其发病机制可能与紫外线照射所引起的基因突变有关,一些研究发现紫外线照射可以引起细胞DNA的破坏,从而使细胞DNA翻译时“C”被“T”所取代,而引起基因突变,从而为皮肤肿瘤的发生提供了分子学基础。同时对于临床病例的调查发现:接受阳光照射较多地区的MCC发病率明显高于接受阳光照射较少地区的MCC发病率 [7] [8] 。
3. 临床特点
MCC的发病主要有以下特征:MCC主要生长于皮下组织或真皮内,表现为红褐色或蓝色的皮肤或皮下结节,肿瘤大小主要在3~6 cm,据相关报道肿瘤最大者直径可达23 cm。其表皮受累较少见,但也有部分患者出现皮肤表面溃烂 [9] [10] 。由于早期临床表现与皮肤色素斑相似,所以容易被误诊或忽略而影响治疗。Heath等在2008年提出将MCC的临床表现归纳为“AEIOU”5元音法表示:A(asymptomatic):无明显临床表现;E (expanding rapidly):病情进展速度快;I (immune suppression):伴有免疫抑制;O (old than age 50):年龄 > 50岁;U (UV-exposed):紫外线经常暴露部位皮肤变白。后续在195例患者的研究中,89%呈现了AEIOU特征中的3种以上 [11] 。约超过50%的MCC患者发生在紫外线直接照射的头部、面部以及颈部。约40%发生在四肢,大约10%的肿瘤分布在躯干或者臀部。其中面部以及颈部的肿物较容易被患者察觉,接受治疗也相对较早。MCC患者的中位年龄为66岁,根据目前相关报道,患者年龄最小者为7岁,年龄最大者为97岁,发病以60~70岁以上的老年人为主,少部分患者为50岁以前的年轻人 [9] [10] 。关于Merkel细胞癌的分期的共识指南见表1。
4. 组织学及免疫组织化学特点
MMC的确诊主要依靠病理组织学检查及免疫组化证实。镜下特点:肿瘤以真皮为中心,常累及皮

Table 1. American Society of Cancer Joint Committee (AJCC) Consensus Guidelines on Merkel Cell Staging
表1. 美国癌症学会联合委员会(AJCC)关于Merkel细胞癌分期的共识指南
下脂肪,约10%患者肿瘤可向表皮内扩散,包括Pautrier样微脓肿形成,偶尔肿瘤细胞可完全局限于表皮,此种情况注意不要误诊为恶性黑色素瘤。MCC的组织学形态分为3种类型 [8] :中间型、梁状型和小细胞型,以中间型最常见,小细胞型最少见,恶性程度也最高。三种形态特点大致如下:中间型约占组织形态的50%以上,其组成以结节状和弥漫片状分布的嗜碱性肿瘤细胞为主,伴空泡化、淡染核,含有小核仁,部分癌组织伴有神经节细胞分化以及淋巴上皮样变的特征,也可伴有广泛凋亡及灶状坏死。梁状型较常见,约占三种形态的25%,其重要组成为纤细带状一致的细胞,部分可见核重叠现象(核膜平行排列)。小细胞型则以深染的“燕麦细胞样”浸润及破碎明显的细胞为其特征,此种MCC应当注意与肺小细胞癌相鉴别。通常癌组织呈实性巢状或弥漫片状分布于真皮内,而肿瘤周边主要是彩带样或缎带小梁状结构,有时也可见呈梭形的癌细胞,此种情况下中间型细胞常混于其中。MCC免疫组化表现特征:免疫表型均显示神经内分泌特征,神经丝蛋白(NF)、嗜铬素A (CgA)、Syn、NSE、CD56常阳性,而S-100少见阳性,CK20为Merkel细胞癌敏感而特异的标志物。部分肿瘤细胞表达CD117,近1/3表达CD99 [12] 。
5. 治疗及预后
目前对于MCC的治疗,以手术切除为主,辅助放疗及化疗。手术切除应选择扩大切除,切除范围应据肿瘤边缘1~2 cm [11] [13] 。大量的回顾性分析发现:术后辅助放疗以及化疗可降低患者肿瘤复发的可能,而且放疗效果将优于化疗效果 [14] 。在一项回顾性分析中还发现对于I、II期患者术后辅助放化疗比单纯手术治疗更有益于提高患者的远期生存率,但对于III期患者无论术后放疗或者化疗都无法改善患者远期生存率。临床指南上也不推荐对晚期患者行化学治疗 [15] 。临床上的化疗方案主要为:CAV (C环磷酰胺,A阿霉素,E长春新碱)。目前一些相关的免疫治疗如白细胞介素(IL) 12及干扰素(IFN)γ也应用于该病的治疗,但效果还有待于进一步明确。MCC具有高度侵袭性,易转移和复发,预后极差,约37%的MCC患者会发生局部淋巴结转移,6%~12%的MMC患者会发生远处转移。复发率约40%,超过1/3 MCC患者会因此病死亡,其死亡率是恶性黑色素瘤死亡率的2倍 [16] 。关于预后的影响因素较多,目前研究发现除去临床分期之外,男性、高龄,维生素D缺乏以及免疫抑制等因素提示着预后不良,另外一些研究发现CD117以及PI3K的过度表达也是预后差的因素 [17] 。
文章引用
王明建,李思源,赵鹏,孟庆海,林惠忠. Merkel细胞癌1例并文献回顾
A Case of Merkel Cell Carcinoma and the Review of Literature[J]. 外科, 2018, 07(02): 61-66. https://doi.org/10.12677/HJS.2018.72010
参考文献
- 1. Toker, C. (1972) Trabecular Carcinoma of the Skin. Archives of Dermatology, 105, 107-110. https://doi.org/10.1001/archderm.1972.01620040075020
- 2. Houben, R., Schrama, D. and Becker, J.C. (2009) Molecular Pathogenesis of Merkel Cell Carcinoma. Experimental Dermatology, 18, 193-198. https://doi.org/10.1111/j.1600-0625.2009.00853.x
- 3. Zwan, J.M.V.D., Trama, A., Otter, R., et al. (2013) Rare Neuro-endocrine Tumours: Results of the Surveillance of Rare Cancers in Europe Project. European Journal of Cancer, 49, 2565-2578. https://doi.org/10.1016/j.ejca.2013.02.029
- 4. Fitzgerald, T.L., Dennis, S., Kachare, S.D., et al. (2015) Dramatic Increase in the Incidence and Mortality from Merkel Cell Carcinoma in the United States. American Surgeon, 81, 802-806.
- 5. Youlden, D.R., Soyer, H.P., Youl, P.H., et al. (2014) Incidence and Survival for Merkel Cell Carcinoma in Queensland, Australia, 1993-2010. Jama Dermatology, 150, 864-872. https://doi.org/10.1001/jamadermatol.2014.124
- 6. Spurgeon, M.E. and Lambert, P.F. (2013) Merkel Cell Polyomavirus: A Newly Discovered Human Virus with Oncogenic Potential. Virology, 435, 118-130. https://doi.org/10.1016/j.virol.2012.09.029
- 7. Bickle, K., Glass, L.F., Messina, J.L., et al. (2004) Merkel Cell Carcinoma: A Clinical, Histopathologic, and Immunohistochemical Review. Seminars in Cutaneous Medicine & Surgery, 23, 46-53. https://doi.org/10.1016/S1085-5629(03)00087-7
- 8. Smith, K. and Skelton, H. (2003) Overview of Merkel Cell Carci-noma and Recent Advances in Research. International Journal of Dermatology, 42, 669-676. https://doi.org/10.1046/j.1365-4362.2003.01913.x
- 9. Mott, R.T., Smoller, B.R. and Morgan, M.B. (2004) Merkel Cell Carci-noma: A Clinicopathologic Study with Prognostic Implications. Journal of Cutaneous Pathology, 31, 217-223. https://doi.org/10.1111/j.0303-6987.2004.00149.x
- 10. Bahadir, S., Cobanoglu, U., Alpay, K., et al. (2004) Merkel Cell Carcinoma. Current Treatment Options in Oncology, 5, 195-199. https://doi.org/10.1007/s11864-004-0011-9
- 11. Tai, P. (2015) A Practical Update of Surgical Management of Merkel Cell Carcinoma of the Skin. Isrn Surgery, 2013, 850797.
- 12. Garneski, K.M., Warcola, A.H., Feng, Q., et al. (2009) Merkel Cell Polyomavirus Is More Frequently Present in North American than Australian Merkel Cell Carcinoma Tumors. Journal of Investigative Dermatology, 129, 246-248. https://doi.org/10.1038/jid.2008.229
- 13. (2004) National Comprehensive Cancer Network Dermatofibrosarcoma Protu-berans and Merkel Cell Carcinoma. Merkel Cell Carcinoma. Clinical Practice Guidelines in Oncology. Journal of the National Comprehensive Cancer Network, 2, 80.
- 14. Garneski, K.M. and Nghiem, P. (2007) Merkel Cell Carcinoma Adjuvant Therapy: Current Data Support Radiation But Not Chemotherapy. Journal of the American Academy of Dermatology, 57, 166-169. https://doi.org/10.1016/j.jaad.2007.03.011
- 15. Vargo, J.A., Ghareeb, E.R., Balasubramani, G.K., et al. (2017) RE: Adju-vant Radiation Therapy and Chemotherapy in Merkel Cell Carcinoma: Survival Analyses of 6908 Cases from the National Cancer Data Base. Journal of the National Cancer Institute, 109. https://doi.org/10.1093/jnci/djx052
- 16. Heath, M., Jaimes, N., Lemos, B., et al. (2008) Clinical Characteristics of Merkel Cell Carcinoma at Diagnosis in 195 Patients: The “AEIOU” Features. Journal of the American Academy of Dermatology, 58, 375-381. https://doi.org/10.1016/j.jaad.2007.11.020
- 17. Ba, V.A.S., Camp, E.R. and Lentsch, E.J. (2012) Merkel Cell Carcinoma: Identification of Prognostic Factors Unique to Tumors Located in the Head and Neck Based on Analysis of SEER Data. Laryn-goscope, 122, 1283-1290. https://doi.org/10.1002/lary.23222
NOTES
*通讯作者