Advances in Clinical Medicine
Vol.
12
No.
03
(
2022
), Article ID:
49573
,
9
pages
10.12677/ACM.2022.123304
荷瘤门脉流域完全切除对肝细胞癌患者术后生存影响的荟萃分析
师恒鑫*,安斌斌*,朱晓颖,任秋洋,齐攀,寇文豪,李淑文,王粟,樊海宁#
青海大学附属医院肝胆胰外科青海大学研究生院,青海 西宁
收稿日期:2022年2月21日;录用日期:2022年3月13日;发布日期:2022年3月23日

摘要
目的:选择接受肝切除的肝细胞癌,评价解剖性肝切除和非解剖性肝切除对患者预后的影响。方法:应用计算机检索PubMed、Cochrane Library、EMBASE数据库中2010年1月至2021年3月关于肝细胞癌接受解剖性肝切除与非解剖性切除的文章,对患者一般特征、肿瘤特征、手术特征和远期预后进行系统评价。结果:共纳入11项病例对照研究,2471例患者,其中解剖性肝切除组1252例,非解剖性肝切除组1219例。和非解剖性肝切除组比较,解剖性肝切除组基线特征为吲哚青绿15分钟滞留率数值更小、手术时间更长、术中失血量更多。长期预后方面,与非解剖性肝切除组相比,解剖性肝切除组获得了更好的术后5年无瘤生存率[比值比(OR) = 1.40,95% CI:1.06~1.84,P = 0.016],而在5年总体生存率方面,两种术式无显著差异[OR = 1.23, 95% CI: 0.96~1.59, P = 0.106]。结论:解剖性肝切除对于降低肝细胞癌患者远期复发显著优于非解剖性肝切除。
关键词
肝细胞癌,解剖性肝切除,非解剖性肝切除,预后

Effect of Complete Removal of the Tumor-Bearing Portal Territory on Prognosis of Patients with Hepatocellular Carcinoma: A Systematic Review and Meta-Analysis
Hengxin Shi*, Binbin An*, Xiaoying Zhu, Qiuyang Ren, Pan Qi, Wenhao Kou, Shuwen Li, Su Wang, Haining Fan#
Department of Hepatobiliary-Pancreatic Surgery, The Affiliated Hospital of Qinghai University, Graduate School of Qinghai University, Xining Qinghai
Received: Feb. 21st, 2022; accepted: Mar. 13th, 2022; published: Mar. 23rd, 2022

ABSTRACT
Objective: Hepatocellular carcinoma undergoing hepatectomy was selected to evaluate the effect of anatomical hepatectomy and non-anatomical hepatectomy on the prognosis of patients. Methods: PubMed, EMBASE and Cochrane Library databases were searched for articles on AR and NAR from January 2010 to March 2021. Meta-analysis was performed on patient characteristics, tumor characteristics, surgical characteristics and long-term prognosis. Results: A total of 11 case-control studies were included in this study, including 2471 patients: there were 1252 cases in the AR group and 1219 cases in the NAR group. Compared with the NAR group, the AR group had lower ICG R15 value, longer operation time and higher intraoperative blood loss. Compared with the NAR group, the AR group achieved a better postoperative 5-year disease-free survival rate [OR = 1.40, 95% CI: 1.06~1.84, P = 0.016], but there was no significant difference in the 5-year overall survival rate between the two groups [OR = 1.23, 95% CI: 0.96~1.59, P = 0.106]. Conclusions: AR is significantly better than NAR for reducing long-term recurrence in HCC.
Keywords:Hepatocellular Carcinoma, Anatomic Resection, Non-Anatomic Resection, Prognosis

Copyright © 2022 by author(s) and Hans Publishers Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY 4.0).
http://creativecommons.org/licenses/by/4.0/


1. 引言
肝切除术目前是肝细胞癌(Hepatocellular carcinoma, HCC)的主要根治性手段,肝切除术根据手术方式分为荷瘤门脉流域完全切除,即解剖性切除术(anatomic resection, AR)和不规则切除,即非解剖性切除术(non-anatomic resection, NAR)。两种术式对患者预后影响长期存在争议。一些研究证明了AR在HCC术后无瘤生存率(disease-free survival, DFS)或总体生存率(overall survival, OS)方面的优势 [1] [2],而有一些研究则发现这两种术式在HCC术后DFS或OS方面没有显著差异 [3] [4]。因此,本研究的目的是进一步评价AR和NAR对HCC患者术后生存的影响。
2. 资料与方法
2.1. 文献检索
在一名经验丰富的专家指导下,两名研究人员采用文献报道的“PICOS”原则 [5] 进行独立检索,继而确定最终的检索策略。检索数据库包括PubMed、Embase、Cochrane Library;使用“Hepatocellular carcinoma”、“anatomic resection”、“non-anatomic resection”的英文相关关键词和医学主题标题的检索策略。将检索时间设定在2011年1月1日至2021年3月31日。
2.2. 文献筛选
文献纳入标准为:1) 肝细胞癌行AR与NAR的比较;2) 随机对照试验、队列研究和病例对照研究;3) 英文和中文文献;4) 报道了5年的无瘤生存率(disease-free survival, DFS)和总体生存率(overall survival, OS)。排除标准为:1) 不相关文献;2) 重复文献;3) 非对照研究,如综述、荟萃分析和病例报告等;4) 生存数据未报告或无法提取的文献。当需要补充数据时,会通过电子邮件联系相应的作者,请求提供。如果一项研究之后是一项更综合的研究,则选择最新的研究。这些研究是根据作者、机构、随访时间和纳入人群来确定的。两名评审员通过讨论解决文献筛选中的异议。
2.3. 数据提取和质量评价
提取的研究数据制成表格,包括患者特征、肿瘤特征、手术特征、病理特征和生存数据。数据提取和质量评估由两名评审员独立完成,最终汇总成达成一致的数据结果。采用纽卡斯尔-渥太华量表(Newcastle-Ottawa Scale, NOS)评估每项研究的质量。该量表总分为9分,文献得分越高,说明质量越好。7分及7分以上的得分被认为是高质量研究。排除NOS低于5分的低质量研究。
2.4. 数据分析和偏倚评估
系统评价使用R 软件(版本4.0.3;http://www.r-project.org/),以术后DFS和OS作为结果指标进行荟萃分析。二分类变量分析采用Mantel-Haenszel或D-L方法,采用固定效应模型(p > 0.1时)或随机效应模型(p < 0.1时)进行比较,效应尺度为比值比(odds ratio, OR)及95%置信区间。连续变量用均值 ± 标准差即( )描述,用倒方差法或D-L法进行分析,采用固定效应模型(p > 0.1时)或随机效应模型(p < 0.1时)进行比较,效应尺度为均数差(mean difference, MD)及95%置信区间;当研究报告连续变量为中位数和极差或四分位数时,用Luo等 [6] 和Wan等 [7] 提出的公式估计均数和标准差。总疗效用Z检验确定。双侧P值 < 0.05被认为差异具有统计学意义。
通过观察漏斗图的对称性和Egger’s检验来评估发表偏倚。通过异质性检验的p值(定性)和I2 (定量)来检验统计异质性。当p < 0.1时,认为研究间存在异质性,反之,则研究间不存在异质性;当I2 = 0时,认为研究间不存在异质性;当I2 < 25%时,认为研究间存在轻度异质性;当25% ≤ I2 < 50%时,认为研究间存在中度异质性;当50% ≤ I2 < 75%时,认为研究间存在高度异质性。由于这项系统评价是基于在纳入标准上不完全相同的病例对照研究,所以进行了敏感性分析以确认结果的稳定性。每删除一项研究,就进行一项新的系统评价。如果异质性显著降低或研究结果发生改变,则认为本研究是异质性的主要来源,应对本研究进行进一步评价。
本荟萃分析完全遵循Cochrane干预性试验系统评价手册(Cochrane Handbook for Systematic Reviews of Interventions) [8],系统评价和荟萃分析优先报告的条目(the Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines, PRISMA) [9] 和系统评价评估清单量表(A Measurement Tool to Assess systematic Reviews checklist, AMSTAR)研究方案是事先确定的,并由评价者严格执行。
3. 结果
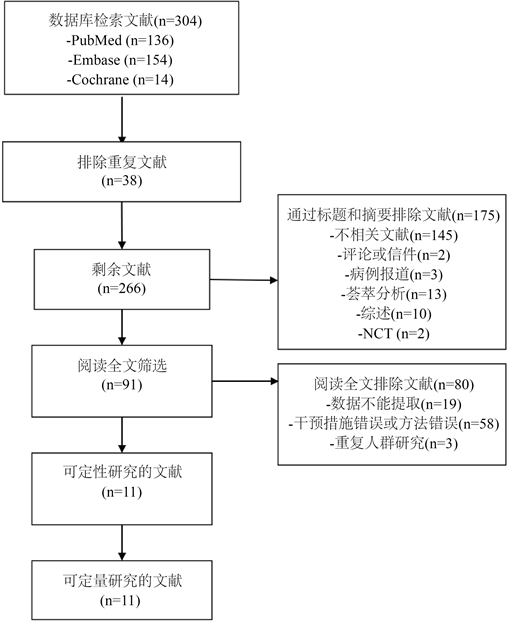
1) 文献选择和文献特征:如图1所示,共检索到304篇文献,经过3个层次筛选。在第1层,排除重复、较旧版本或不相关文献,排除综述、系统评价、信件、个案报告、评论、国家临床试验等研究;在第2层,如果研究报告生存数据,则摘要进入后续水平筛选;在第3层,阅读全文,了解AR和NAR之间的生存数据和基线数据。经过三个层次的筛选,最后有11项研究 [1] [2] [3] [4] [10] - [16] 纳入系统评价,包括日本6项,中国2项,韩国1项,还有2项分别来自日本和韩国、意大利和中国的联合研究(表1)。11项研究共包括2471例患者,其中AR组1252例(50.67%),NAR组1219 (49.33%)。纳入的研究全部属于病例对照研究,各研究NOS评分均为7分。
 注:NCT为国家临床试验。
注:NCT为国家临床试验。
Figure 1. Flow diagram of study selection
图1. 文献筛选流程图

Table 1. The demographics of the included studies
表1. 纳入研究的人口统计数据
注:NOS为纽卡斯尔-渥太华量表;AR为解剖性切除术;NAR为非解剖性切除术。
2) 人群基线特征:如表2所示,AR组与NAR组在性别分布 [1] [2] [3] [4] [10] - [16]、年龄 [1] [2] [3] [4] [10] - [16]、乙肝感染率 [1] [2] [3] [4] [10] - [16]、丙肝感染 [1] [3] [4] [10] - [15]、肝硬化 [1] [2] [3] [10] - [16]、Child-Pugh A级占比 [1] [2] [4] [10] - [16]、肿瘤大小 [1] [2] [3] [4] [10] - [15]、微血管侵犯发生率 [1] [4] [10] [11] [13] [14] [15]、高分化肿瘤占比 [1] [2] [3] [10] [12] [13] [14] [15] 和输血率 [1] [2] [4] [10] [12] [13] [14] [15] [16] 方面差异无统计学意义(均p > 0.05);但是AR组患者具有更小的吲哚青绿15分钟滞留率(indocyanine green retention rate at 15 min,ICG R15)数值 [1] [2] [3] [4] [10] [12] [13] [14] [15],且需要更长的手术时间 [1] [2] [3] [4] [10] [12] [13] [14] [15] [16] 和较多的术中失血 [1] [2] [3] [4] [10] [12] [13] [14] [15] [16],组间差异有统计学意义(均p < 0.05)。
Table 2. Brief results of comparison between AR and NAR group
表2. AR组与NAR组肝细胞癌患者的基线特征
注:AR为解剖性切除术;NAR为非解剖性切除术;ICG R15为吲哚青绿15 min滞留率;DFS为无瘤生存率;OS为总体生存率。
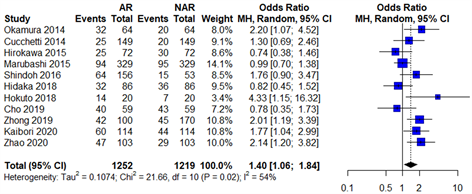
3) 长期生存结果:如图2所示,术后5年 [1] [2] [3] [4] [10] - [16] 的DFS,AR组相比于NAR组均明显获益,组间差异有统计学意义(均p < 0.05)。术后5年 [1] [2] [3] [4] [10] - [16] 的OS,AR组与NAR组间差异无统计学意义(p > 0.05)。
 (a)
(a)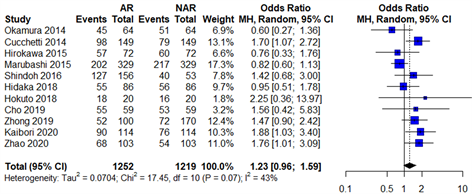 (b)注:AR为解剖性切除术;NAR为非解剖性切除术;Odds Ratio为比值比;Random effect model为随机效应模型;Heterogeneity为异质性。
(b)注:AR为解剖性切除术;NAR为非解剖性切除术;Odds Ratio为比值比;Random effect model为随机效应模型;Heterogeneity为异质性。
Figure 2. Forest plot comparing the long-term survival of patients with hepatocellular carcinoma in AR group and NAR group. (a) Forest plot for comparison of 5-year disease-free survival after surgery; (b) Forest plot for comparison of 5-year overall survival after surgery
图2. AR组与NAR组肝细胞癌患者长期生存比较的森林图。(a) 术后5年无瘤生存率比较的森林图;(b) 术后5年总体生存率比较的森林图
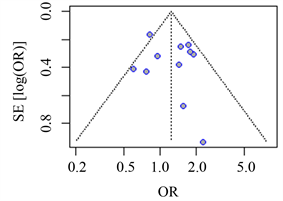 (a) (b)注:AR为解剖性切除术;NAR为非解剖性切除术;OR为比值比。
(a) (b)注:AR为解剖性切除术;NAR为非解剖性切除术;OR为比值比。
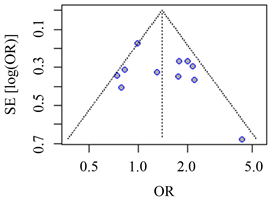
Figure 3. The funnel plot for the comparison of the long-term survival of hepatocellular carcinoma patients in the AR group and the NAR group. (a) The funnel plot for the comparison of the 5-year postoperative disease-free survival results; (b) The funnel plot for the comparison of the 5-year postoperative overall survival results
图3. AR组与NAR组肝细胞癌患者长期生存比较的漏斗图。(a) 术后5年无瘤生存率结果比较的漏斗图;(b) 术后5年总体生存率结果比较的漏斗图
4) 发表偏倚和敏感性分析:两组比较的各项生存指标的森林图有相对较多的重叠,代表性森林图如图2所示,这意味着纳入研究的异质性可接受。两组比较的漏斗图大致对称(图3),Egger’s检验结果,术后5年的DFS (p = 0.307),术后5年的OS的(p = 0.491)均表明发表偏倚很小。敏感性分析显示,术后5年的DFS和5年OS的结果稳定性良好。
4. 讨论
目前肝癌的治疗方式主要分为3大类,局部治疗、区域性治疗和全身性治疗。局部治疗包括肝切除、消融治疗和肝移植;区域性治疗主要包括经肝动脉化疗栓塞术(transcatheter arterial chemoembolization, TACE)和钇90微球栓塞治疗;全身性治疗包括传统全身化学药物治疗、靶向治疗和免疫药物治疗 [17]。在过去的十年中,肝切除术在肝细胞癌治疗中的适应症持续扩大。一般来说,对于非转移性疾病和基础肝功能正常的患者或代偿性肝硬化且无门脉高压的患者,应考虑肝切除术 [18]。肝切除术分为AR与NAR。根据日本学者Makuuchi等 [19] 的描述,AR是系统性地沿着门静脉将一个肝段及其所属门静脉分支支配的区域连同动脉等一并切除,包括肝叶、肝段、亚肝段等的切除术。NAR指切除原发肿瘤及距离原发肿瘤一定距离内的肝组织,不考虑肝叶、肝段的肝切除术。由于肝细胞癌主要是通过侵犯门静脉分支进行转移 [20],因此,AR理论上能有效降低肝切除术后的复发,从而提高术后生存率。但是,对于两种手术的选择一直存在争议。因此,本研究将进一步探究两种手术方式对肝细胞癌患者术后长期生存的影响。
由于AR切除的肝体积较NAR大,外科医生更倾向对肝储备功能更好的HCC患者行AR。因此,既往的很多研究在组间基线中存在较大的差异,为了克服这种缺陷,本研究纳入的文献都是使用倾向性匹配评分(Propensity Score Matching, PSM)的研究。 在组间基线比较中,仅ICG 15数值、术中失血量和手术时长在两组间存在差异,但是,AR组和NAR间的ICG 15数值尽管存在差异,但是其数值差异非常小(MD: −0.76, 95% CI: −1.17~−0.35),对HCC术后的长期生存可能影响较小。
本研究结果显示,AR组较NAR组在5年的DFS方面明显获益。既往的大部分荟萃分析 [21] [22] [23] 研究结果和本研究一致,而仅有一项荟萃分析 [24] 得出不同结论。笔者分析认为,首先,AR完全切除荷瘤门脉流域能有效清除微血管侵犯,从而降低术后复发,因此,AR对存在微血管侵犯的HCC更能有效降低其术后复发,当研究纳入的HCC患者微血管侵犯率较低时,这种优势可能体现不出(本研究纳入的HCC微血管侵犯发生率为39.4%);其次,基于日本全国数据库的一项研究发现 [25],当肿瘤小于2 cm时,AR和NAR两种术式对HCC的术后DFS的影响无显著差异,可能是由于肿瘤小于2 cm时,无论哪种术式都能有效清除微血管侵犯,因此,当纳入文献中小于2 cm的HCC占比过较高时,可能对研究结果会产生决定性影响;最后,尽管该研究也纳入的是PSM文献,但基线仍然可能存在显著差异,其文中也未进行组间基线的详细比较。
理论上讲,AR降低HCC术后复发,从而能提高术后的OS,但是,本研究结果显示,AR组和NAR组间的术后5年OS无显著差异。既往的一些荟萃分析和本研究结果一致 [22] [23] [26],而另一些和本研究结果不同 [24] [27] [28],既往对5年术后OS的研究结果差异较大。这可能主要由于术后复发接受再治疗的方法,个体差异较大。复发后可接受的再治疗方式包括手术切除、肝移植、介入治疗和射频消融、靶向和免疫治疗等,这些复发后的治疗都会对术后OS造成影响,而且术后时间越长,这些后续治疗的影响越明显。
AR组较NAR组需要更长的手术时间和较多的失血量,这与AR手术对外科技术要求更高有关,本研究中显示,手术时长(I2 = 79%)和术中失血量(I2 = 75%)在各研究之间存在高度异质性,这也说明了不同外科医生对AR的掌握熟练程度差异很大。
然而,本研究存在几点局限性:1) 本研究纳入的人群在肿瘤大小、分期上没有严格限定,可能对研究结果的准确性造成一定影响;2) 本荟萃分析纳入的研究均是回顾性病例对照试验,因此,仍需前瞻性随机对照研究来验证本结论。
5. 结论
综上所述,与NAR相比较,尽管AR需要更长的手术时间和较多的出血量,但是AR对于降低患者术后复发具有明显优势。所以,对于剩余肝体积充足的HCC,解剖性肝切除更值得推荐。未来,设计良好的前瞻性随机对照临床研究,按肿瘤分期进行分层研究,有助于进一步准确评价AR和NAR对于肝细胞癌治疗的临床价值。
利益冲突
所有作者均声明不存在利益冲突。
作者贡献声明
课题设计:樊海宁、师恒鑫和安斌斌
文献检索:师恒鑫、安斌斌
文献筛选:朱晓颖、任秋洋
数据提取:齐攀、寇文豪
文献质量评价:李淑文、王粟
数据分析:师恒鑫
论文起草由师恒鑫完成;樊海宁完成最终版本的修订
文章引用
师恒鑫,安斌斌,朱晓颖,任秋洋,齐 攀,寇文豪,李淑文,王 粟,樊海宁. 荷瘤门脉流域完全切除对肝细胞癌患者术后生存影响的荟萃分析
Effect of Complete Removal of the Tumor-Bearing Portal Territory on Prognosis of Patients with Hepatocellular Carcinoma: A Systematic Review and Meta-Analysis[J]. 临床医学进展, 2022, 12(03): 2116-2124. https://doi.org/10.12677/ACM.2022.123304
参考文献
- 1. Kaibori, M., Yoshii, K., Hasegawa, K., et al. (2020) Impact of Systematic Segmentectomy for Small Hepatocellular Carcinoma. Journal of Hepato-Biliary-Pancreatic Sciences, 27, 331-341. https://doi.org/10.1002/jhbp.720
- 2. Zhao, H., Ding, W.Z., Wang, H., et al. (2020) Prognostic Value of Precise Hepatic Pedicle Dissection in Anatomical Resection for Patients with Hepatocellular Carcinoma. Medicine, 99, Article No. e19475. https://doi.org/10.1097/MD.0000000000019475
- 3. Marubashi, S., Gotoh, K., Akita, H., et al. (2015) Anatomical versus Non-Anatomical Resection for Hepatocellular Carcinoma. British Journal of Surgery, 102, 776-784. https://doi.org/10.1002/bjs.9815
- 4. Hidaka, M., Eguchi, S., Okuda, K., et al. (2020) Impact of Anatomical Resection for Hepatocellular Carcinoma with Microportal Invasion (vp1): A Multi-Institutional Study by the Kyushu Study Group of Liver Surgery. Annals of Surgery, 271, 339-346. https://doi.org/10.1097/SLA.0000000000002981
- 5. Methley, A.M., Campbell, S., Chew-Graham, C., et al. (2014) PICO, PICOS and SPIDER: A Comparison Study of Specificity and Sensitivity in Three Search Tools for Qualitative Systematic Reviews. BMC Health Services Research, 14, Article No. 579. https://doi.org/10.1186/s12913-014-0579-0
- 6. Luo, D., Wan, X., Liu, J., et al. (2018) Optimally Estimating the Sample Mean from the Sample Size, Median, Mid-Range, and/or Mid-Quartile Range. Statistical Methods in Medical Research, 27, 1785-1805. https://doi.org/10.1177/0962280216669183
- 7. Wan, X., Wang, W., Liu, J., et al. (2014) Estimating the Sample Mean and Standard Deviation from the Sample Size, Median, Range and/or Interquartile Range. BMC Medical Research Methodology, 14, Article No. 135. https://doi.org/10.1186/1471-2288-14-135
- 8. Higgins, J.P.T., Thomas, J., Chandler, J., et al. (2021) Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (Updated February 2021). Cochrane. http://www.training.cochrane.org/handbook
- 9. Moher, D., Shamseer, L., Clarke, M., et al. (2015) Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 Statement. Systematic Reviews, 4, Article No. 1. https://doi.org/10.1186/2046-4053-4-1
- 10. Okamura, Y., Ito, T., Sugiura, T., et al. (2014) Anatomic versus Nonanatomic Hepatectomy for a Solitary Hepatocellular Carcinoma: A Case-Controlled Study with Propensity Score Matching. Journal of Gastrointestinal Surgery, 18, 1994-2002. https://doi.org/10.1007/s11605-014-2646-6
- 11. Cucchetti, A., Qiao, G.L., Cescon, M., et al. (2014) Anatomic versus Nonanatomic Resection in Cirrhotic patients with Early Hepatocellular Carcinoma. Surgery, 155, 512-521. https://doi.org/10.1016/j.surg.2013.10.009
- 12. Hirokawa, F., Kubo, S., Nagano, H., et al. (2015) Do Patients with Small Solitary Hepatocellular Carcinomas without Macroscopically Vascular Invasion Require Anatomic Resection? Propensity Score Analysis. Surgery, 157, 27-36. https://doi.org/10.1016/j.surg.2014.06.080
- 13. Shindoh, J., Makuuchi, M., Matsuyama, Y., et al. (2016) Complete Removal of the Tumor-Bearing Portal Territory Decreases Local Tumor Recurrence and Improves Disease-Specific Survival of Patients with Hepatocellular Carcinoma. Journal of Hepatology, 64, 594-600. https://doi.org/10.1016/j.jhep.2015.10.015
- 14. Hokuto, D., Nomi, T., Yasuda, S., et al. (2018) Does Anatomic Resection Improve the Postoperative Outcomes of Solitary Hepatocellular Carcinomas Located on the Liver Surface? Surgery, 163, 285-290. https://doi.org/10.1016/j.surg.2017.08.024
- 15. Cho, C.W., Choi, G.S., Kim, J.M., et al. (2019) Long-Term Oncological Outcomes of Laparoscopic Liver Resection for Solitary Hepatocellular Carcinoma: Comparison of Anatomical and Nonanatomical Resection Using Propensity Score Matching Analysis. Journal of Laparoendoscopic & Advanced Surgical Techniques, 29, 752-758. https://doi.org/10.1089/lap.2018.0600
- 16. Zhong, X.P., Zhang, Y.F., Mei, J., et al. (2019) Anatomical versus Non-Anatomical Resection for Hepatocellular Carcinoma with Microscope Vascular Invasion: A Propensity Score Matching Analysis. Journal of Cancer, 10, 3950-3957. https://doi.org/10.7150/jca.32592
- 17. 刘允怡. 肝细胞癌治疗的新发展[J]. 中华消化外科杂志, 2022, 21(1): 15-18. https://doi.org/10.3760/cma.j.cn115610-20220107-00020
- 18. Orcutt, S.T. and Anaya, D.A. (2018) Liver Resection and Surgical Strategies for Management of Primary Liver Cancer. Cancer Control, 25, Article ID: 1073274817744621. https://doi.org/10.1177/1073274817744621
- 19. Makuuchi, M., Hasegawa, H. and Yamazaki, S. (1985) Ultrasonically Guided Subsegmentectomy. Surgery, Gynecology and Obstetrics, 161, 346-350.
- 20. Nakashima, T. and Kojiro, M. (1986) Pathologic Characteristics of Hepatocellular Carcinoma. Seminars in Liver Disease, 6, 259-266. https://doi.org/10.1055/s-2008-1040608
- 21. Cucchetti, A., Cescon, M., Ercolani, G., et al. (2012) A Comprehensive Meta-Regression Analysis on Outcome of Anatomic Resection versus Nonanatomic Resection for Hepatocellular Carcinoma. Annals of Surgical Oncology, 19, 3697-3705. https://doi.org/10.1245/s10434-012-2450-z
- 22. Moris, D., Tsilimigras, D.I., Kostakis, I.D., et al. (2018) Anatomic versus Non-Anatomic Resection for Hepatocellular Carcinoma: A Systematic Review and Meta-Analysis. European Journal of Surgical Oncology, 44, 927-938. https://doi.org/10.1016/j.ejso.2018.04.018
- 23. Jiao, S., Li, G., Zhang, D., et al. (2020) Anatomic versus Non-Anatomic Resection for Hepatocellular Carcinoma, Do We Have an Answer? A Meta-Analysis. International Journal of Surgery, 80, 243-255. https://doi.org/10.1016/j.ijsu.2020.05.008
- 24. Famularo, S., Ceresoli, M., Giani, A., et al. (2021) Is It Just a Matter of Surgical Extension to Achieve the Cure of Hepatocarcinoma? A Meta-Analysis of Propensity-Matched and Randomized Studies for Anatomic versus Parenchyma-Sparing Liver Resection. Journal of Gastrointestinal Surgery, 25, 94-103. https://doi.org/10.1007/s11605-019-04494-5
- 25. Eguchi, S., Kanematsu, T., Arii, S., et al. (2008) Comparison of the Outcomes between an Anatomical Subsegmentectomy and a Non-Anatomical Minor Hepatectomy for Single Hepatocellular Carcinomas Based on a Japanese Nationwide Survey. Surgery, 143, 469-475. https://doi.org/10.1016/j.surg.2007.12.003
- 26. Sun, Z., Li, Z., Shi, X.L., et al. (2021) Anatomic versus Non-Anatomic Resection of Hepatocellular Carcinoma with Microvascular Invasion: A Systematic Review and Meta-Analysis. Asian Journal of Surgery, 44, 1143-1150. https://doi.org/10.1016/j.asjsur.2021.02.023
- 27. Chen, J., Huang, K.,Wu, J., et al. (2011) Survival after Anatomic Resection versus Nonanatomic Resection for Hepatocellular Carcinoma: A Meta-Analysis. Digestive Diseases and Sciences, 56, 1626-1633. https://doi.org/10.1007/s10620-010-1482-0
- 28. Ye, J.Z., Miao, Z.G., Wu, F.X., et al. (2012) Recurrence after Anatomic Resection versus Nonanatomic Resection for Hepatocellular Carcinoma: A Meta-Analysis. Asian Pacific Journal of Cancer Prevention, 13, 1771-1777. https://doi.org/10.7314/APJCP.2012.13.5.1771
NOTES
*同等贡献。
#通讯作者Email: fanhaining@medmail.com.cn