Asian Case Reports in Surgery
Vol.
07
No.
03
(
2018
), Article ID:
27809
,
14
pages
10.12677/ACRS.2018.73004
Comparison of Perioperative and Functional Outcomes between Standard Laparoscopic and Robotic-Assisted Radical Prostatectomy: A Systemic Review and Meta-Analysis
Shuchang Huang, Minbo Yan, Wenfei Lian
Department of Urology, The Fifth Affiliated Hospital of Sun Yat-sen University, Zhuhai Guangdong
![]()
Received: Nov. 1st, 2018; accepted: Nov. 22nd, 2018; published: Nov. 29th, 2018

ABSTRACT
[Objective] The goal of this study was to perform a systemic review and meta-analysis to evaluate the perioperative and functional outcomes between laparoscopic radical prostatectomy (LRP) and robotic-assisted radical prostatectomy (RARP). [Methods] A literature search of EMBASE, MEDLINE, PubMed, and Cochrane Library databases was conducted. We selected randomized controlled trials (RCTs) and non-randomized comparative studies (including prospective and retrospective studies) comparing perioperative and functional outcomes of both LRP and RARP, and meta-analysis was applied using the Review Manager 5.3 software. [Results] Twenty-four studies were identified in the literature search, including 2 RCTs, 7 prospective studies, and 15 retrospective studies. LRP and RARP showed similarity in the operative time, catheterization duration, in-hospital stay, and overall complication rate (P > 0.05). However, blood loss and transfusion rate were lower in RARP (P < 0.05). Moreover, RARP was associated with significantly improved outcomes for continence and potency rates to those of LRP at 3, 6, and 12 months postoperatively (P < 0.05). [Conclusion] RARP was associated with lower blood loss and transfusion rate and much greater functional outcomes in contrast to LRP.
Keywords:Prostate Cancer, Radical Prostatectomy, Laparoscopy, Robotics, Meta-Analysis
机器人辅助腹腔镜与标准腹腔镜前列腺癌根治术疗效比较的Meta分析
黄书畅,延敏博,练文飞
中山大学附属第五医院泌尿外科,广东 珠海
![]()
收稿日期:2018年11月1日;录用日期:2018年11月22日;发布日期:2018年11月29日

摘 要
[目的] 评价机器人辅助腹腔镜前列腺癌根治术(RARP)与标准腹腔镜前列腺癌根治术(LRP)治疗局限性前列腺癌的临床疗效。[方法] 检索EMBASE、MEDLINE、PubMed、Cochrane图书馆,并选择有关LRP与RARP临床疗效的随机对照研究(RCTs)和非随机对照研究(包括前瞻和回顾性研究),应用系统评价软件Rev Man5.3进行Meta分析。[结果] 通过文献检索共纳入24个研究,包括2个RCTs、7个前瞻性和15个回顾性研究。Meta分析表明:两组在手术时间、导尿管留置时间、住院时间和总体并发症发生率方面无统计学差异(P > 0.05)。但在失血量、输血率、术后3、6、12月的控尿和勃起功能恢复方面,RARP组明显优于LRP组(P < 0.05)。[结论] 与LRP相比,RARP在局限性前列腺癌的手术治疗中出血量少、输血率低,且在术后控尿和勃起功能恢复上较LRP更有优势。
关键词 :前列腺癌,根治性前列腺切除术,腹腔镜,机器人,Meta分析

Copyright © 2018 by authors and Hans Publishers Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/


1. 引言
前列腺癌是老年男性最常见的恶性肿瘤之一,随着我国人口老龄化,前列腺癌在我国的发病率和死亡率逐年升高。根治性前列腺切除术是临床局限性前列腺癌患者唯一的手术选择 [1] 。随着微创外科技术的迅猛发展,根治性前列腺切除术最主要的微创手术方式包括标准腹腔镜根治性前列腺切除术(laparoscopic radical prostatectomy, LRP)和机器人辅助腹腔镜根治性前列腺切除术(robotic-assisted radical prostatectomy, RARP)。与LRP相比,RARP具有更好的视觉放大效果、3D手术视角、操作精细灵活等优点,在世界范围内的应用越来越广泛 [2] 。
近年来,有两项关于LRP与RARP临床疗效的随机对照研究(randomized controlled trails, RCTs)证实:RARP在控尿和勃起功能恢复上具有明显优势 [3] [4] 。但是,其他系统性回顾研究又表明二者在围手术期及功能恢复上无明显差异 [2] [5] [6] 。因此,我们采用Meta分析方法对相关的临床对照研究进行定量评价,以探讨二者在围手术期和术后功能恢复方面的疗效差异,为今后临床决策提供一定的理论参考。
2. 资料与方法
2.1. 文献检索策略
我们检索EMBASE、MEDLINE、PubMed、Cochrane图书馆,并选择有关LRP与RARP临床疗效的对照研究(截止至2016年7月)。检索中以“radical prostatectomy, laparoscopic, robotic”为英文检索词,三者之间逻辑操作符为“AND”。并对入选文献的参考文献进行二次检索。
2.2. 纳入/排除标准
纳入标准:1) 研究类型:检索上述数据库中有关LRP和RARP治疗前列腺癌的临床对照研究文献,研究设计为RCTs和非随机对照研究(包括前瞻性和回顾性研究)。2) 病例类型:首次治疗的临床局限性前列腺癌患者,且均有前列腺癌手术指征。3) 观察指标:两种手术方式的手术时间、失血量、输血率、导尿管留置时间、住院时间、总体并发症发生率、术后3、6、12月的控尿和勃起功能恢复率。
排除标准:1) 非对照研究;2) 研究设计有缺陷、质量差,统计学方法错误且无法修正或原始数据提供不完整;3) 晚期前列腺癌或合并其他恶性肿瘤患者,入组前接受过内分泌治疗、放疗、化疗等,且治疗导致不同预后者;4) 对于重复报告,只纳入发表日期较新的研究。
2.3. 数据提取
根据纳入/排除标准筛选文献,两位研究者单独提取数据记录在提前制定的数据表中,并交叉审核,意见不一致时通过讨论决定或者由第三者来裁决。针对纳入研究的特征,提取的数据包括:第一作者、发表年份、国家、研究设计及证据水平;患者特征指标包括:年龄、体重指数(body mass index, BMI)和术前前列腺特性抗原(prostate-specific antigen, PSA)值;围手术期指标包括:手术时间、失血量、输血率、导管留置时间、住院时间和并发症发生率;功能恢复指标包括:控尿和勃起功能。使用Cochrane系统评价员手册对纳入的RCTs进行偏倚风险评价。
2.4. 统计学分析
采用英国牛津大学Cochrane协作网推荐的系统评价软件RevMan5.3进行Meta分析。连续性变量采用均数差值(MD)、二分类变量采用比值比(OR)及它们的95%可信区间(CI)对结果进行描述,P < 0.05为差异有统计学意义。通过Cochrane Q检验来评估纳入研究的异质性,若P > 0.05,I2 < 50%,认为各研究间不具异质性,采用固定效应模型,用Mantel-Haenszel法(M-H)分析;若P < 0.05,I2 > 50%,认为各研究间存在异质性,采用随机效应模型,用Inverse-Variance法分析。
3. 结果
3.1. 文献检索结果
文献筛选过程见图1。通过初筛纳入文献3103篇,阅读文献标题和摘要后排除2933篇。初步纳入文献170篇,通过阅读全文,按照图1所示原因排除了148篇文献,同时对纳入文献的参考文献进行二次检索,纳入2篇文献。最终,共有24篇文献纳入本Meta分析 [3] [4] [7] - [28] 。在上述24篇文献中,21篇报道了围手术期结果和并发症 [3] [4] [7] - [13] [15] - [23] [26] [27] [28] ,15篇报道了术后尿控恢复情况 [3] [4] [7] [9] [10] [12] [15] [17] [18] [19] [21] [23] [26] [27] [28] ,13篇报道了术后勃起功能恢复情况 [3] [4] [9] [10] [15] [17] [18] [19] [21] [23] [26] [27] [28] 。
3.2. 研究的基本特性
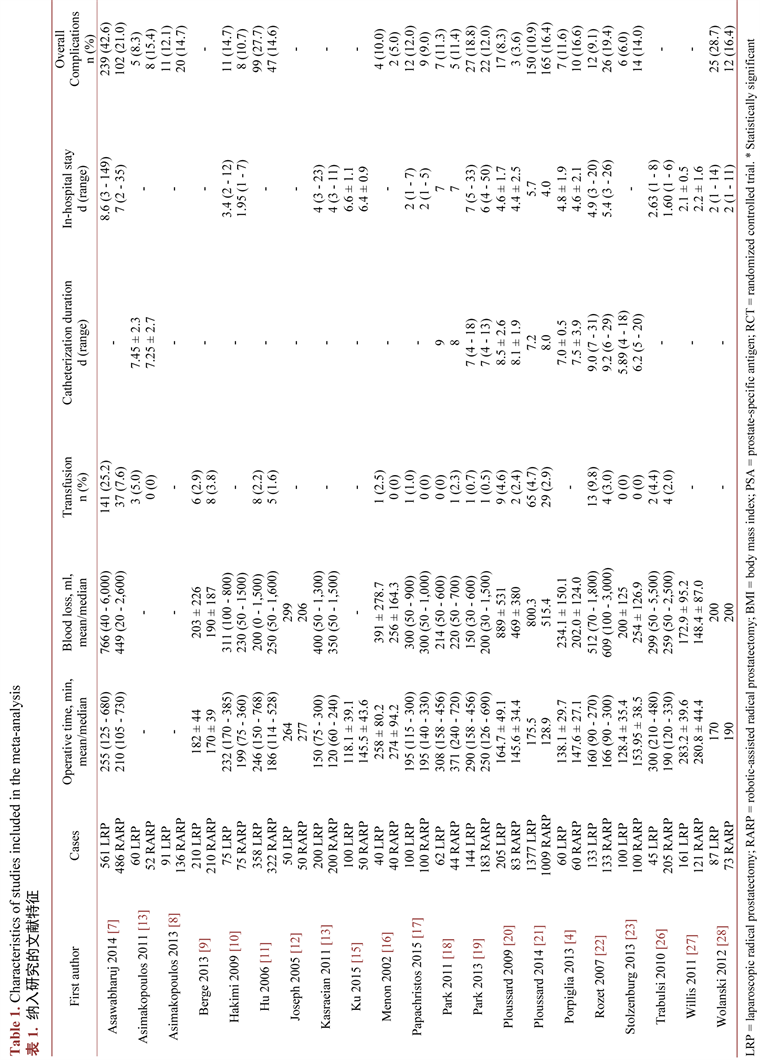
本研究共纳入9178例患者,5064例患者行LRP,4114例患者行RARP。在纳入的24个研究中,有2个随机对照研究(证据级别1b) [3] [4] ,7个前瞻性研究(证据级别2b) [8] [9] [14] [16] [20] [21] [23] ,7个病例对照的回顾性研究(证据级别3b) [7] [11] [15] [17] [19] [22] [28] ,以及8个研究病例系列或使用历史病例作为对照的回顾性研究(证据级别4) [10] [12] [13] [18] [24] [25] [26] [27] 。两项RCTs研究的偏倚风险为中等(图2)。纳入研究的基本特征详见表1。
![]()
Figure 1. Flowchart of the meta-analysis
图1. 文献筛选流程图
![]()
Figure 2. Risk of bias for eligible randomized controlled trials
图2. 随机对照试验偏倚风险总结图
3.3. 围手术期结果及并发症
LAP和RARP两组在手术时间、失血量、输血率、导尿管留置时间、住院时间和总体并发症发生率
的比较详见表2。Meta分析显示:两组在手术时间上无明显差异(MD: −5.31分; 95% CI: −19.41 to 8.80; P = 0.46) (图3(A)),而在失血量(MD: 75.94 ml; 95% CI: 6.95 to 144.94; P = 0.03)和输血率(OR: 2.08; 95% CI: 1.33 to 3.26; P = 0.001)上RARP组则明显降低(图3(B)、图3(C))。
两组间导尿管留置时间无明显差异(MD: 0.20天; 95% CI: −0.23 to 0.62; P = 0.37),且具有较低的异质性(P = 0.30; I2 = 18%) (图3(D))。同样,两组间住院时间的差异也无统计学意义(MD: 0.07 day; 95% CI: −0.13 to 0.26; P = 0.52),采用固定效应模型,Q检验无异质性(P = 0.54; I2 = 0%) (图3(E))。
此外,LRP组总体并发症发生率为18.3% (632/3453),而RARP组为15.6% (453/2896),Meta分析显示两组并发症发生率比较无明显差异(OR: 1.13; 95% CI: 0.74 to 1.74; P = 0.57) (图3(F))。
3.4. 功能恢复情况
3.4.1. 控尿功能恢复
LRP和RARP两组术后3、6和12月的控尿恢复情况详见表3。在报道控尿恢复的15个研究中,有11个将不用尿垫或没有漏尿定义为控尿恢复,而其他4个则认为不用或每天仅使用1片尿垫为控尿恢复。两者相比,前者对控尿的定义更加严格。因此,我们将更控尿定义更为严格的研究纳入Meta分析 [3] [7] [9] [10] [12] [15] [17] [19] [21] [27] [28] 。
LRP术后3、6和12月的尿失禁发生率分别为:56.8% (1263/2224),44.9% (1038/2310)和29.8% (772/2593)。而RARP术后3、6和12月的尿失禁发生率分别为:44.9% (801/1783),27.7% (520/1, 879)和 20.8% (442/2, 126)。Meta分析显示:在术后3 (OR: 1.73; 95% CI: 1.30 to 2.32; P = 0.0002)、6 (OR: 2.20; 95% CI: 1.60 to 3.04; P < 0.00001)和12月(OR: 1.62; 95% CI: 1.20 to 2.17; P = 0.001)的比较中,RARP术后控尿恢复均具有明显优势(图4(A)-(C))。
3.4.2. 勃起功能恢复
LRP和RARP两组术后3、6和12月的勃起功能恢复情况详见表3。勃起功能恢复定义为性交时阴茎充分的勃起或IIEF-5评分>17分。在13个报道术后勃起功能恢复的研究中,保留双侧勃起神经8个 [3] [9] [10] [17] [21] [26] [27] [28] ,保留单侧或双侧的5个 [4] [15] [18] [19] [23] 。其中有1个研究患者术前勃起功能不详,将该研究剔除 [15] 。
LRP术后3、6和12月的勃起功能障碍发生率分别为:82.5% (1091/1323),74.5% (872/1170)和62.7% (801/1278)。而RARP术后3、6和12月的勃起功能障碍发生率分别为:67.4% (809/1201),54.5% (581/1067)和40.4% (499/1234)。Meta分析显示:在术后3 (OR: 2.20; 95% CI: 1.48 to 3.28; P = 0.0001)、6(OR: 2.34; 95% CI: 1.43 to 3.84; P = 0.0008)和12月(OR: 2.20; 95% CI: 1.41 to 3.43; P = 0.0005),RARP术后勃起功能恢复优于LRP (图4(D)-(F))。
3.5. 发表偏倚
评价发表偏倚,最好是纳入10个研究以上绘制漏斗图 [29] 。因围手术期指标中仅输血率及总体并发症发生率纳入的研究大于10篇,绘制漏斗图呈不对称图形,因此发表偏倚不能排除(图5)。手术时间、出血量、导尿管留置时间、住院时间及术后控尿和勃起功能恢复情况纳入的研究均小于10篇,故未做漏斗图评价发表偏倚。
4. 讨论
借助机器人辅助系统,外科医师能够更加精细、灵活的进行复杂的腔镜手术。与LRP相比,RARP学习曲线更短,操作更为精细,有望成为前列腺癌根治术的金标准 [30] 。但是,现阶段RARP明显优于LRP的确切证据尚不充分。迄今为止,只有2个比较RARP和LRP的RCTs显示:在术后尿控和勃起功能恢复方面RARP优于LRP [3] [4] 。但是,其他系统评价及Meta分析又表明二者在围手术期及功能恢复上无明显差异 [2] [5] [6] 。目前,关于二者在围手术期和术后功能恢复方面比较的Meta分析仍比较少。因此,本研究采用Meta分析方法对二者进行评价,以期为临床前列腺癌的治疗决策提供循证医学依据。
评价前列腺癌围手术期的指标主要有:住院时间、出血量、输血率、导尿管留置时间、住院时间和总体并发症发生率等。在我们收集的研究资料中,LRP组手术时间约118.1 min~308 min,而RARP组约120 min~371 min,两组间没有明显差异。而RARP组在出血量和输血率方面更有优势。这与Novara等 [31] 在2012年发表的Meta分析基本相符。
两组在导尿管留置时间和住院时间上基本相似。大多数进行LRP或RARP的患者术后均留置导尿管7~10天。住院天数则因不同国家的医疗保险体系和文化背景差异而不同。在美国和澳大利亚,患者一般在术后2天内出院 [10] [17] [26] [27] [28] ,而在欧洲患者住院时间一般在4~6天 [4] [13] [20] [21] [22] 。亚洲国家的住院时间最长,一般在一周左右 [7] [15] [18] [19] 。
![]()
Figure 5. Funnel plot of the studies for transfusion rate and overall complication rate
图5. 输血率及总体并发症发生率纳入文献的漏斗图
一般来说,围手术期并发症代表着手术方式的安全性。LRP组总体并发症发生率为18.3%,而RARP组为15.6%,两组间差异无明显统计学意义。Agarwal等 [32] 报道了2005年至2009年间在三级转诊中心进行RARP手术的3317例患者,其总体并发症率为9.8%,且大多数均发生在术后30天内,证实RARP手术安全可行。Schmitges等 [33] 比较了近期(2006~2007)和早期(2001~2005)进行微创前列腺癌根治术的并发症发生率,发现近期并发症发生率明显降低。因此,在我们看来,外科医师的手术经验在很大程度上会影响手术的并发症,而与手术方式关系不大。
控尿和勃起功能的恢复是前列腺癌根治术后患者最关切的问题。在我们的Meta分析中,将不用尿垫或没有漏尿定义为控尿恢复,LRP组术后3、6和12月的尿失禁发生率分别为:56.8%,44.9%和29.8%。而RARP组术后3、6和12月的尿失禁发生率分别为:44.9%,27.7%和 20.8%。这提示RARP术后控尿的恢复可能更早。同样,我们发现RARP在术后勃起功能恢复方面也优于LRP。我们的结论与最近发表的仅纳入两个RCTs的Meta分析结论基本一致 [34] 。
但是,在比较二者术后功能恢复方面有些要点也是不容忽略的。首先,诸如膀胱颈保护、神经保留技术、耻骨前列腺韧带保留、后层及前层肌筋膜重建等手术技术,在很大程度上影响了术后控尿和勃起功能的恢复 [35] 。其次,大多数研究的术后功能恢复随访资料是通过面谈方式采集的,在评价功能结果时会导致明显的偏差。第三,由于目前对控尿和勃起功能恢复尚缺乏标准的定义,根据不同的定义就会得出不同的结论。因此,在评估LRP和RARP术后功能恢复方面需警惕上述情况的存在。
作为一个具有光明前景的手术方式,RARP已经在世界范围内广泛应用。年青一代的泌尿外科医师需要尽快掌握该技术,并在今后的工作中加以熟练应用。当然,RARP也有其自身的缺陷,比如设备故障,缺少长期的肿瘤随访数据以及经费昂贵等 [36] 。在我们Meta分析中,解释结果时也存在一定的局限性。首先,纳入的研究中,只有两个是RCTs,其他多数研究质量较低。其次,在评估相关结果时缺乏标准和精确的方法。
综上所述,与LRP相比,RARP在前列腺癌的治疗中有更少的出血量及输血率,且在术后控尿和勃起功能恢复上更有优势。由于现阶段纳入的对照研究质量较低,文章结论存在一定的局限性,今后仍需要更多的高质量、多中心的RCTs研究来证实。
文章引用
黄书畅,延敏博,练文飞. 机器人辅助腹腔镜与标准腹腔镜前列腺癌根治术疗效比较的Meta分析
Comparison of Perioperative and Functional Outcomes between Standard Laparoscopic and Robotic-Assisted Radical Prostatectomy: A Systemic Review and Meta-Analysis[J]. 亚洲外科手术病例研究, 2018, 07(03): 17-30. https://doi.org/10.12677/ACRS.2018.73004
参考文献
- 1. Heidenreich, A., Bastian, P.J., Bellmunt, J., et al., European Association of Urology (2014) EAU Guidelines on Prostate Cancer. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent-Update 2013. European Urology, 65, 124-137. https://doi.org/10.1016/j.eururo.2013.09.046
- 2. Robertson, C., Close, A., Fraser, C., et al. (2013) Relative Effectiveness of Robot-Assisted and Standard Laparoscopic Prostatectomy as Alternatives to Open Radical Prostatectomy for Treatment of Localised Prostate Cancer: A Systematic Review and Mixed Treatment Comparison Meta-Analysis. BJU International, 112, 798-812. https://doi.org/10.1111/bju.12247
- 3. Asimakopoulos, A.D., Pereira Fraga, C.T., Annino, F., et al. (2011) Randomized Comparison between Laparoscopic and Robot-Assisted Nerve-Sparing Radical Prostatectomy. The Journal of Sexual Medicine, 8, 1503-1512. https://doi.org/10.1111/j.1743-6109.2011.02215.x
- 4. Porpiglia, F., Morra, I., Lucci Chiarissi, M., et al. (2013) Randomised Controlled Trial Comparing Laparoscopic and Robot-Assisted Radical Prostatectomy. European Urology, 63, 606-614. https://doi.org/10.1016/j.eururo.2012.07.007
- 5. Ficarra, V., Novara, G., Artibani, W., et al. (2009) Retropubic, Laparoscopic, and Robot-Assisted Radical Prostatectomy: A Systematic Review and Cumulative Analysis of Comparative Studies. European Urology, 55, 1037-1063. https://doi.org/10.1016/j.eururo.2009.01.036
- 6. Moran, P.S., O'Neill, M., Teljeur, C., et al. (2013) Robot-Assisted Radical Prostatectomy Compared with Open and Laparoscopic Approaches: A Systematic Review and Meta-Analysis. International Journal of Urology, 20, 312-321. https://doi.org/10.1111/iju.12070
- 7. Asawabharuj, K., Ramart, P., Nualyong, C., et al. (2014) Comparison of Urinary Continence Outcome between Robotic Assisted Laparoscopic Prostatectomy versus Laparoscopic Radical Prostatectomy. Journal of the Medical Association of Thailand, 97, 393-398.
- 8. Asimakopoulos, A.D., Miano, R., Di Lorenzo, N., et al. (2013) Laparoscopic versus Robot-Assisted Bilateral Nerve-Sparing Radical Prostatectomy: Comparison of Pentafecta Rates for a Single Surgeon. Surgical Endoscopy, 27, 4297-4304. https://doi.org/10.1007/s00464-013-3046-9
- 9. Berge, V., Berg, R.E., Hoff, J.R., et al. (2013) A Prospective Study of Transition from Laparoscopic to Robot-Assisted Radical Prostatectomy: Quality of Life Outcomes after 36-Month Follow-Up. Urology, 81, 781-786. https://doi.org/10.1016/j.urology.2013.01.017
- 10. Hakimi, A.A., Blitstein, J., Feder, M., et al. (2009) Direct Comparison of Surgical and Functional Outcomes of Robotic-Assisted versus Pure Laparoscopic Radical Prostatectomy: Single-Surgeon Experience. Urology, 73, 119-123. https://doi.org/10.1016/j.urology.2008.08.491
- 11. Hu, J.C., Nelson, R.A., Wilson, T.G., et al. (2006) Perioperative Complications of Laparoscopic and Robotic Assisted Laparoscopic Radical Prostatectomy. The Journal of Urology, 175, 541-546. https://doi.org/10.1016/S0022-5347(05)00156-4
- 12. Joseph, J.V., Vicente, I., Madeb, R., et al. (2005) Robot-Assisted vs Pure Laparoscopic Radical Prostatectomy: Are There Any Differences? BJU International, 96, 39-42. https://doi.org/10.1111/j.1464-410X.2005.05563.x
- 13. Kasraeian, A., Barret, E., Chan, J., et al. (2011) Comparison of the Rate, Location and Size of Positive Surgical Margins after Laparoscopic and Robot-Assisted Laparoscopic Radical Prostatectomy. BJU International, 108, 1174-1178. https://doi.org/10.1111/j.1464-410X.2010.10077.x
- 14. Koutlidis, N., Mourey, E., Champigneulle, J., et al. (2012) Robot-Assisted or Pure Laparoscopic Nerve-Sparing Radical Prostatectomy: What Is the Optimal Procedure for the Surgical Margins? A Single Center Experience. International Journal of Urology, 19, 1076-1081. https://doi.org/10.1111/j.1442-2042.2012.03102.x
- 15. Ku, J.Y. and Ha, H.K. (2015) Learning Curve of Robot-Assisted Laparoscopic Radical Prostatectomy for a Single Experienced Surgeon: Comparison with Simultaneous Laparoscopic Radical Prostatectomy. World Journal of Men’s Health, 33, 30-35. https://doi.org/10.5534/wjmh.2015.33.1.30
- 16. Menon, M., Shrivastava, A., Tewari, A., et al. (2002) Laparoscopic and Robot Assisted Radical Prostatectomy: Establishment of a Structured Program and Preliminary Analysis of Outcomes. The Journal of Urology, 168, 945-949. https://doi.org/10.1016/S0022-5347(05)64548-X
- 17. Papachristos, A., Basto, M., Te Marvelde, L., et al. (2015) Laparoscopic versus Robotic-Assisted Radical Prostatectomy: An Australian Single-Surgeon Series. ANZ Journal of Surgery, 85, 154-158. https://doi.org/10.1111/ans.12602
- 18. Park, J.W., Won Lee, H., Kim, W., et al. (2011) Comparative Assessment of a Single Surgeon’s Series of Laparoscopic Radical Prostatectomy: Conventional versus Robot-Assisted. Journal of Endourology, 25, 597-602. https://doi.org/10.1089/end.2010.0229
- 19. Park, B., Kim, W., Jeong, B.C., et al. (2013) Comparison of Oncological and Functional Outcomes of Pure versus Robotic-Assisted Laparoscopic Radical Prostatectomy Performed by a Single Surgeon. Scandinavian Journal of Urology, 47, 10-18. https://doi.org/10.3109/00365599.2012.696137
- 20. Ploussard, G., Xylinas, E., Paul, A., et al. (2009) Is Robot Assistance Affecting Operating Room Time Compared with Pure Retroperitoneal Laparoscopic Radical Prostatectomy? Journal of Endourology, 23, 939-943. https://doi.org/10.1089/end.2008.0521
- 21. Ploussard, G., De la Taille, A., Moulin, M., et al. (2014) Comparisons of the Perioperative, Functional, and Oncologic Outcomes after Robot-Assisted versus Pure Extraperitoneal Laparoscopic Radical Prostatectomy. European Urology, 65, 610-619. https://doi.org/10.1016/j.eururo.2012.11.049
- 22. Rozet, F., Jaffe, J., Braud, G., et al. (2007) A Direct Comparison of Robotic Assisted versus Pure Laparoscopic Radical Prostatectomy: A Single Institution Experience. The Journal of Urology, 178, 478-482. https://doi.org/10.1016/j.juro.2007.03.111
- 23. Stolzenburg, J.U., Qazi, H.A., Holze, S., et al. (2013) Evaluating the Learning Curve of Experienced Laparoscopic Surgeons in Robot-Assisted Radical Prostatectomy. Journal of Endourology, 27, 80-85. https://doi.org/10.1089/end.2012.0262
- 24. Tozawa, K., Yasui, T., Umemoto, Y., et al. (2014) Pitfalls of Robot-Assisted Radical Prostatectomy: A Comparison of Positive Surgical Margins between Robotic and Laparoscopic Surgery. International Journal of Urology, 21, 976-979. https://doi.org/10.1111/iju.12492
- 25. Trabulsi, E.J., Linden, R.A., Gomella, L.G., et al. (2008) The Addition of Robotic Surgery to an Established Laparoscopic Radical Prostatectomy Program: Effect on Positive Surgical Margins. The Canadian Journal of Urology, 15, 3994-3999.
- 26. Trabulsi, E.J., Zola, J.C., Gomella, L.G., et al. (2010) Transition from Pure Laparoscopic to Robotic-Assisted Radical Prostatectomy: A Single Surgeon Institutional Evolution. Urologic Oncology, 28, 81-85. https://doi.org/10.1016/j.urolonc.2009.07.002
- 27. Willis, D.L., Gonzalgo, M.L., Brotzman, M., et al. (2012) Comparison of Outcomes between Pure Laparoscopic vs. Robot-Assisted Laparoscopic Radical Prostatectomy: A Study of Comparative Effectiveness Based upon Validated Quality of Life Outcomes. BJU International, 109, 898-905. https://doi.org/10.1111/j.1464-410X.2011.10551.x
- 28. Wolanski, P., Chabert, C., Jones, L., et al. (2012) Preliminary Results of Robot-Assisted Laparoscopic Radical Prostatectomy (RALP) after Fellowship Training and Experience in Laparoscopic Radical Prostatectomy (LRP). BJU International, 110, 64-70. https://doi.org/10.1111/j.1464-410X.2012.11479.x
- 29. Lau, J., Ioannidis, J.P., Terrin, N., et al. (2006) The Case of the Misleading Funnel Plot. BMJ, 333, 597-600. https://doi.org/10.1136/bmj.333.7568.597
- 30. Descazeaud, A., Peyromaure, M. and Zerbib, M. (2007) Will Robotic Surgery Become the Gold Standard for Radical Prostatectomy? European Urology, 51, 9-11. https://doi.org/10.1016/j.eururo.2006.10.007
- 31. Novara, G., Ficarra, V., Rosen, R.C., et al. (2012) Systematic Review and Meta-Analysis of Perioperative Outcomes and Complications after Robot-Assisted Radical Prostatectomy. European Urology, 62, 431-452. https://doi.org/10.1016/j.eururo.2012.05.044
- 32. Agarwal, P.K., Sammon, J., Bhandari, A., et al. (2011) Safety Profile of Robot-Assisted Radical Prostatectomy: A Standardized Report of Complications in 3317 Patients. European Urology, 59, 684-698. https://doi.org/10.1016/j.eururo.2011.01.045
- 33. Schmitges, J., Trinh, Q.D., Abdollah, F., et al. (2011) A Population-Based Analysis of Temporal Perioperative Complication Rates after Minimally Invasive Radical Prostatectomy. European Urology, 60, 564-571. https://doi.org/10.1016/j.eururo.2011.06.036
- 34. Allan, C. and Ilic, D. (2016) Laparoscopic versus Robotic-Assisted Radical Prostatectomy for the Treatment of Localised Prostate Cancer: A Systematic Review. Urologia Internationalis, 96, 373-378. https://doi.org/10.1159/000435861
- 35. Ficarra, V., Novara, G., Rosen, R.C., et al. (2012) Systematic Review and Meta-Analysis of Studies Reporting Urinary Continence Recovery after Robot-Assisted Radical Prostatectomy. European Urology, 62, 405-417. https://doi.org/10.1016/j.eururo.2012.05.045
- 36. Murphy, D.G., Bjartell, A., Ficarra, V., et al. (2010) Downsides of Robot-Assisted Laparoscopic Radical Prostatectomy: Limitations and Complications. European Urology, 57, 735-746. https://doi.org/10.1016/j.eururo.2009.12.021