设为首页
加入收藏
期刊导航
网站地图
首页
期刊
数学与物理
地球与环境
信息通讯
经济与管理
生命科学
工程技术
医药卫生
人文社科
化学与材料
会议
合作
新闻
我们
招聘
千人智库
我要投搞
办刊
期刊菜单
●领域
●编委
●投稿须知
●最新文章
●检索
●投稿
文章导航
●Abstract
●Full-Text PDF
●Full-Text HTML
●Full-Text ePUB
●Linked References
●How to Cite this Article
Hans Journal of Biomedicine
生物医学
, 2012, 2, 11-14
http://dx.doi.org/10.12677/hjbm.2012.21003
Published Online January 2012 (http://www.hanspub.org/journal/hjbm)
An Easily Forgotten Disease in a Malaria-Eliminating
Country: A Report of an Imported Case
Bruno Man-Hon Che ung
1*
, Wen-Hung Lee
2
, Chieh-Jen Wu
3
, Pau-Tien Chen
4
, Kuo-Kuan Chang
5
1
Division of Infectious Diseases, Department of Inte
rnal Medicine, Tainan M
unicipal Hospital, Tainan
2
Division of Endocrinology and Metabolism, Department of Internal Medicine, Tainan Municipal Hospital, Tainan
3
Department of Clinical Laboratory,
Tainan Municipal Hospital, Tainan
4
Department of Medical Emergency,
Tainan Municipal Hospital, Tainan
5
Office of Superintendent, Tainan
Municipal Hospital, Taiwan
Email:
*
mhcheung2005@gmail.com
Received: Oct. 19th, 2011; revised: Nov. 24th, 2011; accepted: Nov. 27th, 2011.
Abstract:
In countries where malaria is endemic, malaria is easily considered in the differential diagnosis for a patient
presenting with fever. However, the diagnosis of malaria is
easily forgotten in malaria-free or malaria-eliminating coun-
tries. Herein, we report an imported case of
Plasmodium falciparum
infection. When the pa
tient was febrile, a thick
blood film examination revealed signet-ring form and earphone-like trophozoites in erythrocytes. After treatment with
intravenous Artesu nate, the patient r ecovered on e week later. We learn that high clinical suspicion and correct d iagnosis
may lead to rapid recovery from
Plasmodium falciparum
infection. With the increase
of international traveling, we
should keep the diagnosis of malaria in mind if a foreigner from an endemic area develops fever, in order to prevent the
disease spreading.
Keywords:
Malaria;
Pla smodium falciparum
; Imported; Arteminisin
疟疾根除国家易被遗忘的传染病:
一个热带疟境外移入病例报告
张文瀚
1*
,李文宏
2
,吴介仁
3
,陈宝田
4
,张国宽
5
1
台南市立医院内科部感染科,台南
2
台南市立医院内科部新陈代谢科,台南
3
台南市立医院临床检验部,台南
4
台南市立医院急诊部,台南
5
台南市立医院院长室,台南
Email:
*
mengyanqiu@hotmail.com
收稿日期:
2011
年
10
月
19
日;修回日期:
2011
年
11
月
24
日;录用日期:
2011
年
11
月
27
日
摘
要:
在疟疾盛行国家,因发烧而求诊的病人,疟疾可能不是主诊断,但在疟疾根除国家地区,因考虑必须
及时治疗的败血症,疟疾很容易被忘记。我们报告一个境外移入的热带疟病例,在病人寒颤、发烧时作厚层血
片检查,很清楚看到呈现耳机状及指环状的疟原虫在红血球里面,经投与青蒿素类
Artesunate
药物静脉注射治
疗,一周后病人顺利康复。因此,我们了解到,对来自疫区的外籍旅客或曾在疫区逗留的本国居民,如因发烧
求诊,应将疟疾列入可能原因之一,以免增加疾病扩散的风险。
关键词:
疟疾;热带疟;境外移入;青蒿素类
1.
引言
疟疾盛行于撒撒哈拉沙漠以南的非洲国家、印
度、大洋洲、中南美洲、及东南亚等国家地区,经由
蚊子传播
[1-3]
。感染人类的疟原虫共有五种:热带疟原
虫
Plasmodium falciparum
、间日疟原虫
Plasmodium
vivax
、卵形疟原虫
Plasmodium ovale
、三日疟原虫
P
*
通讯作者。
Copyright © 2012 Hanspub 11
疟疾根除国家易被遗忘的传染病:一个热带疟境外移入病例报告
lasmodium malariae
、及弥猴疟原虫
Plasmodium know-
lesi
[4-6]
,其中以热带疟最为严重,较易引发重症及致
死,且对传统疟疾治疗药物的抗药性愈来愈高
[7,8]
。在
疟疾根除国家地区,旅游者发烧求诊时,疟疾确诊的
机率约
4%
左右,因考虑必须及时治疗的败血症及其
它更高机率的传染病,疟疾很容易被忘记
[4,9]
。
2.
病例报告
一名
29
岁印度尼西亚籍男性飞机机械工程师,
因公司业务派赴台湾,于
2011
年
4
月
18
日抵达,拟
逗留一个月。翌日因寒颤、发烧、头痛、呕心、呕吐
一次、及全身酸痛无力,到医院急诊室求诊,当时血
压为
122/82 mmHg
、体温
38.5
˚
C
、脉搏每分钟
98
次、
呼吸频率每分钟
18
次、身体理学检查无异状、
胸部
X
光及尿液常规检查为正常,因来自印度尼西亚,疑为
登革热,予以留观,挂蚊帐,并通报疾管局。
4
月
20
日傍晚,接获疾管局通知,登革热检验为阴性结果,
因高烧不退,转住院诊查 ,同时投与静脉注 射
Ceftriaxone
合并口服
Doxycycline
治疗。
4
月
21
日晨
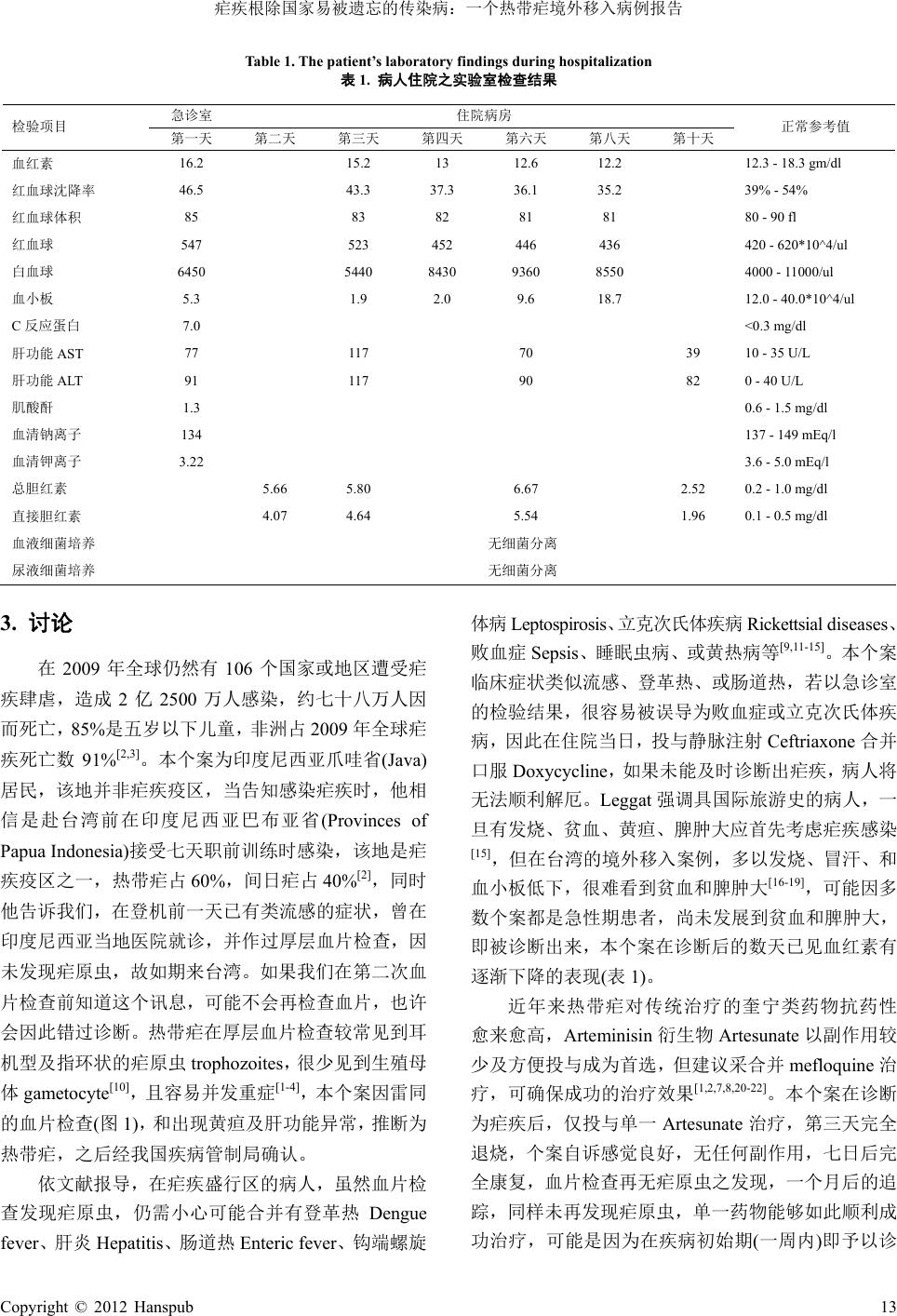
会诊感染科,发现除了发烧及巩膜黄疸外,实验室检
查显示血小板偏低,
CRP
偏高,
及肝功能轻微异常
(
表
1)
,而腹部超音波检查并无肝脾肿大,因来自印度尼
西亚,怀疑是疟疾作祟,嘱咐急检厚层血片检查,上
午
10
时回报是阴性结果。感染科医师再次比对个案
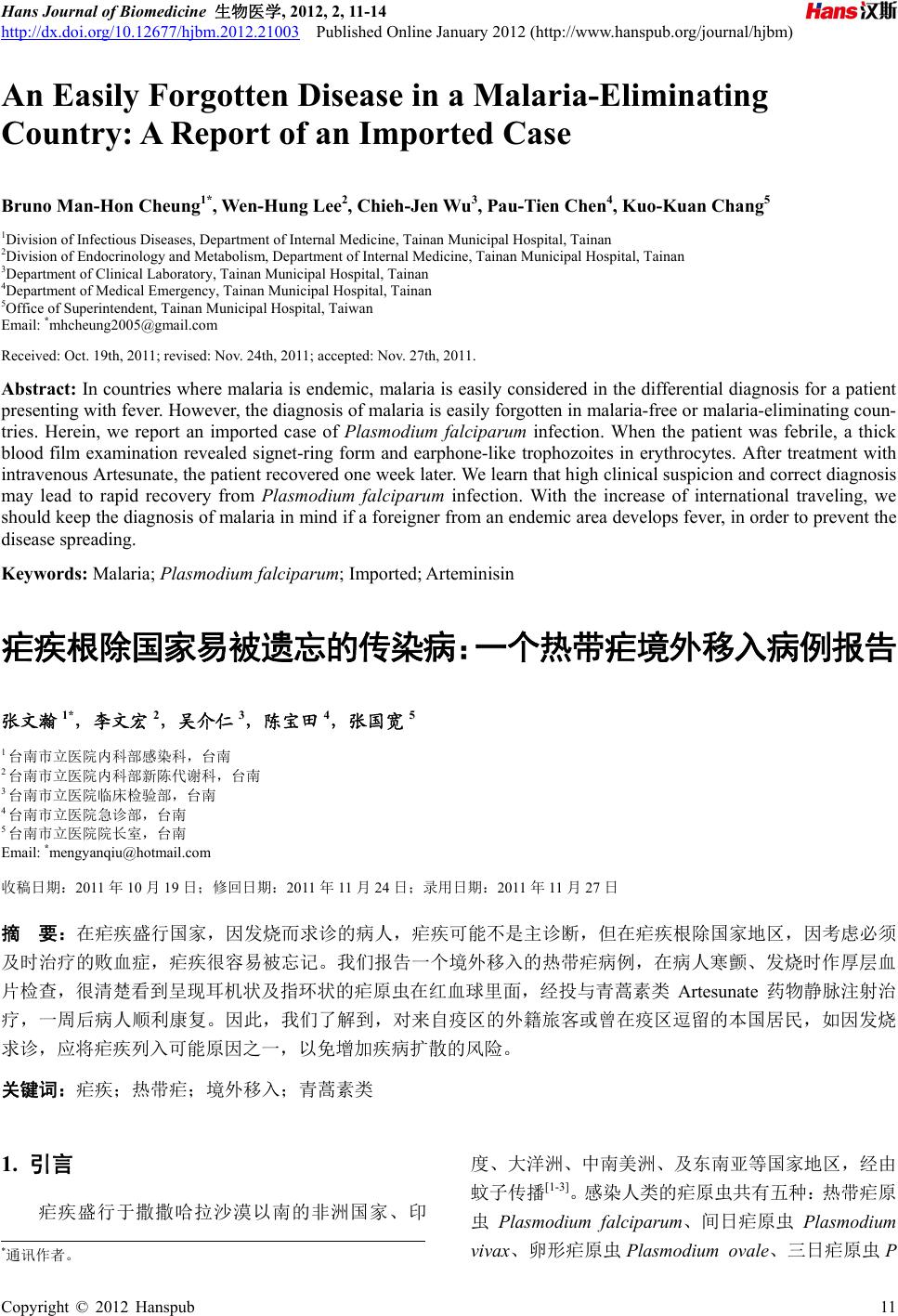
临床情况及实验室各项检查资料,认为疟疾仍需复检
方可排除,嘱咐于寒颤发烧时再作一次厚层血片检
查,下午
2
时,病人高烧发作,血片检查果真发现疟
原虫
(
图
1)
,依血片检查疟原虫的形态,诊断为热带疟,
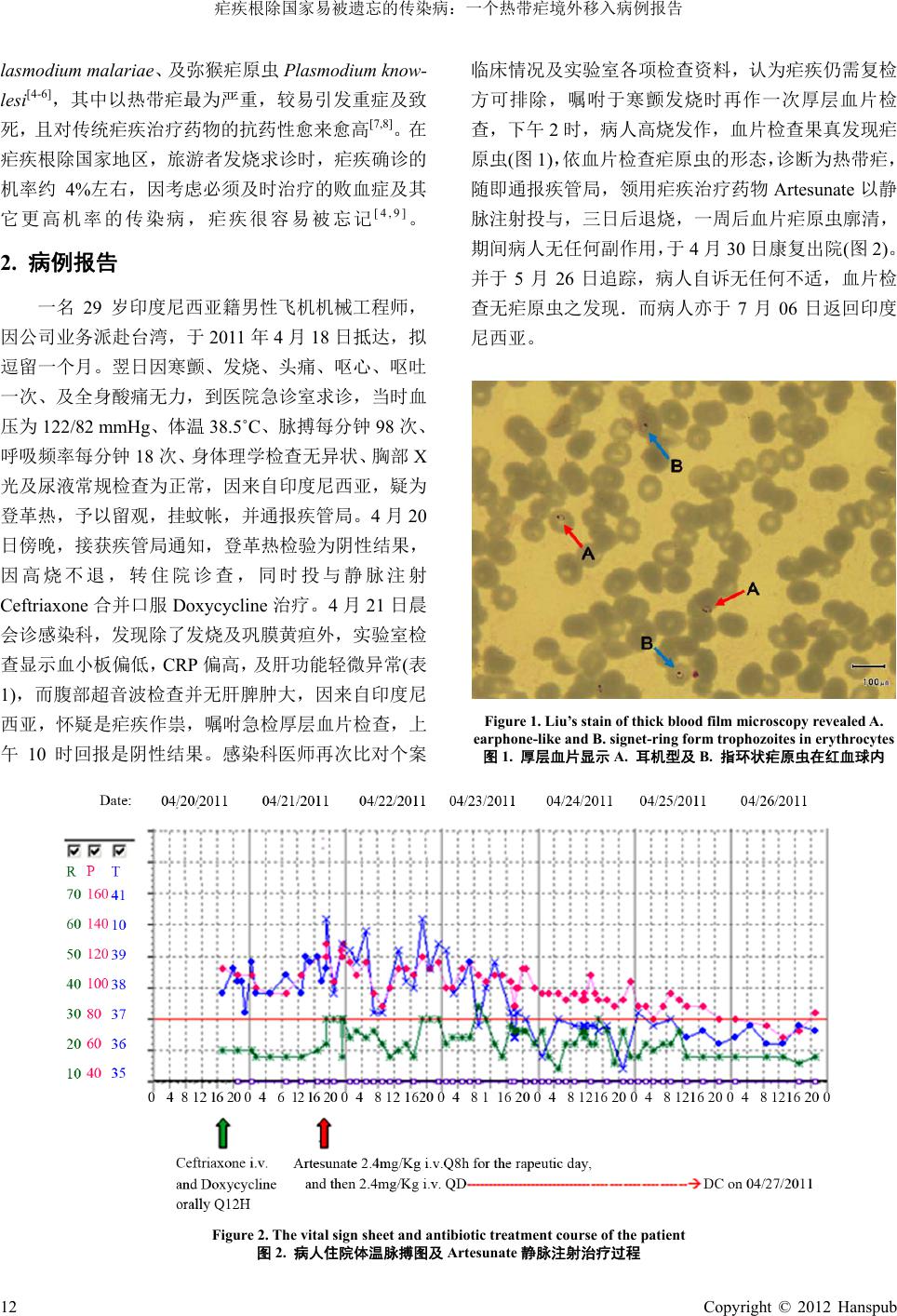
随即通报疾管局,领用疟疾治疗药物
Artesunate
以静
脉注射投与,三日后退烧,一周后血片疟原虫廓清,
期间病人无任何副作用,于
4
月
30
日康复出院
(
图
2)
。
并于
5
月
26
日追踪,病人自诉无任何不适,血片检
查无疟原虫之发现.而病人亦于
7
月
06
日返回印度
尼西亚。
Figure 1. Liu’s stain of thick blood film microscopy revealed A.
earphone-like and B. signet-ring form trophozoites in erythrocytes
图
1.
厚层血片显示
A.
耳机型及
B.
指环状疟原虫在红血球内
Figure 2. The vital sign sheet and antibiotic treatment course of the patient
图
2.
病人住院体温脉搏图及
Artesunate
静脉注射治疗过程
12 Cop
yright © 2012 Hanspub
疟疾根除国家易被遗忘的传染病:一个热带疟境外移入病例报告
Table 1. The patient’s laboratory findings during hospitalization
表
1.
病人住院之实验室检查结果
急诊室
住院病房
检验项目
第一天
第二天
第三天
第四天
第六天
第八天
第十天
正常参考值
血红素
16.2 15.2 13 12.6 12.2 12.3 - 18.3 gm/dl
红血球沈降率
46.5 43.3 37.3 36.1 35.2 39% - 54%
红血球体积
85 83 82 81 81 80 - 90 fl
红血球
547 523 452 446 436 420 - 620*10^4/ul
白血球
6450 5440 8430 9360 8550 4000 - 11000/ul
血小板
5.3 1.9 2.0 9.6 18.7 12.0 - 40.0*10^4/ul
C
反应蛋白
7.0 <0.3 mg/dl
肝功能
AST
77 117 70 39 10 - 35 U/L
肝功能
ALT
91 117 90 82 0 - 40 U/L
肌酸酐
1.3 0.6 - 1.5 mg/dl
血清钠离子
134 137 - 149 mEq/l
血清钾离子
3.22 3.6 - 5.0 mEq/l
总胆红素
5.66 5.80 6.67 2.52 0.2 - 1.0 mg/dl
直接胆红素
4.07 4.64 5.54 1.96 0.1 - 0.5 mg/dl
血液细菌培养
无细菌分离
尿液细菌培养
无细菌分离
3.
讨论
在
2009
年全球仍然有
106
个国家或地区遭受疟
疾肆虐,造成
2
亿
2500
万人感染,约七十八万人因
而死亡,
85%
是五岁以下儿童,非洲占
2009
年全球疟
疾死亡数
91%
[2,3]
。本个案为印度尼西亚爪哇省
(Java)
居民,该地并非疟疾疫区,当告知感染疟疾时,他相
信是赴台湾前在印度尼西亚巴布亚省
(Provinces of
Papua Indonesia)
接受七天职前训练时感染,该地是疟
疾疫区之一,热带疟占
60%
,间日疟占
40%
[2]
,同时
他告诉我们,在登机前一天已有类流感的症状,曾在
印度尼西亚当地医院就诊,并作过厚层血片检查,因
未发现疟原虫,故如期来台湾。如果我们在第二次血
片检查前知道这个讯息,可能不会再检查血片,也许
会因此错过诊断。热带疟在厚层血片检查较常见到耳
机型及指环状的疟原虫
trophozoites
,很少见到生殖母
体
gametocyte
[10]
,且容易并发重症
[1-4]
,本个案因雷同
的血片检查
(
图
1)
,和出现黄疸及肝功能异常,推断为
热带疟,之后经我国疾病管制局确认。
依文献报导,在疟疾盛行区的病人,虽然血片检
查发现疟原虫,仍需小心可能合并有登革热
Dengue
fever
、肝 炎
Hepatitis
、肠 道 热
Enteric fever
、钩端 螺旋
体病
Leptospirosis
、
立克次氏体疾病
Rickettsial diseases
、
败血症
Sepsis
、睡眠虫病、或黄热病等
[9,11-15]
。本个案
临床症状类似流感、登革热、或肠道热,若以急诊室
的检验结果,很容易被误导为败血症或立克次氏体疾
病,因此在住院当日,投与静脉注射
Ceftriaxone
合并
口服
Doxycycline
,如果未能及时诊断出疟疾,病人将
无法顺利解厄。
Leggat
强调具国际旅游史的病人,一
旦有发烧、贫血、黄疸、脾肿大应首先考虑疟疾感染
[15]
,但在台湾的境外移入案例,多以发烧、冒汗、和
血小板低下,很难看到贫血和脾肿大
[16-19]
,可能因多
数个案都是急性期患者,尚未发展到贫血和脾肿大,
即被诊断出来,本个案在诊断后的数天已见血红素有
逐渐下降的表现
(
表
1)
。
近年来热带疟对传统治疗的奎宁类药物抗药性
愈来愈高,
Arteminisin
衍生物
Artesunate
以副作用较
少及方便投与成为首选,但建议采合并
mefloquine
治
疗,可确保成功的治疗效果
[1,2,7,8,20-22]
。本个案在诊断
为疟疾后,仅投与单一
Artesunate
治疗,第三天完全
退烧,个案自诉感觉良好,无任何副作用,七日后完
全康复,血片检查再无疟原虫之发现,一个月后的追
踪,同样未再发现疟原虫,单一药物能够如此顺利成
功治疗,可能是因为在疾病初始期
(
一周内
)
即予以诊
Cop
yright © 2012 Hanspub 13
疟疾根除国家易被遗忘的传染病:一个热带疟境外移入病例报告
断及治疗,感染的疟原虫尚未繁殖出众多的数量。
1965
年世界卫生组织宣布台湾为疟疾根除区
[2,23,24]
,每年仍约有确诊病例
20~30
例,皆为境外移入,
但台湾本土主要传播疟疾的矮小疟蚊
Anopheles
minimus
,在北 台湾及南部的关庙 地区仍可见到牠的
踪迹
[8]
。在台湾曾有介入感染
(introduced infection)
和
当地新染
(indigenous infection)
[8,16-18]
、及诱导感染
(induced infection)
[25]
案例的报告。我们再取个案在急
诊检验室剩余的血液样本作厚层血片检查,亦可发现
疟原虫,表示急诊照护医师在当时若想到疟疾,个案
便可提前两天确诊。幸而个案仍算是及时诊断及治
疗,无机会造成诱导感染
(induced infection)
,经过三
个月观察,亦未发现本土居民有介入感染或当地新染
的案例。
4.
结论
全球迄今仍然有
106
个国家或地区遭受疟疾肆
虐,在国际交通频繁的情况下,对来自疫区的外籍旅
客或曾在疫区逗留的本国居民,如有寒颤、发烧、类
流感症状、并有血小板偏低、或黄疸,应将疟疾列入
可能原因之一。厚层血片检查成本不高,且在短时间
内即可知道结果,在病人寒颤发烧期,加作这项检查
并不会耽误其它鉴别检查或治疗的进行。对高度怀疑
为疟疾的病人,至少要有三次阴性厚层血片检查,方
可排除。但是,一旦忘记疟疾的可能性,就可能带来
疾病在本土散播的危机。
参考文献
(References)
[1]
G. L. Mandell, J. E. Bennett and R. Dolin. Principles and prac-
tice of infectious disease (6th edition). Churchill Livingstone: El se -
vier, 2005: 3122-3126.
[2]
WHO publications: World malaria report 2010.
http://www.who.int/malaria/publications/atoz/9789241564106/e
n/index.html
[3]
Centers for Disease Control, (Taiwan), 2011.
http://www.cdc.gov.tw/lp.asp?ctNode=2622&CtUnit=1508&Bas
eDSD=7&mp=1&nowPage=5&pagesize=15/142211124971.ppt
[4]
Centers for Disease Control and Prevention, USA, 2011.
http://www.cdc.gov/malaria/disease
[5]
B. Singh, L. K. Sung, A. Matusop,
et al
. A large focus of naturally
acquired Plasmodium knowlesi infections in human beings. Lan-
cet, 2004, 9414(363): 1017-1024.
[6]
M. Fi gtre e, R. Lee, L . Ba i n,
et al
. Plasmodium knowlesi i n human,
indonesian borneo. Emerging Infectious Diseases, 2010, 16(4):
672-674.
[7]
Centers for Disease Control and Prevention, USA, 2011.
http://www.cdc.gov/malaria/diagnosis_treatment/diagnosis.html
[8]
Centers for Disease Control (Taiwan). Guideline for malaria
chemoprophylaxis and treatment, 2010.
http://www.cdc.gov.tw/ct.asp?xItem=21932&ctNode=2077&mp
=5
[9]
V. Lo Re III, S. J. Gluck man. Fever in the returned traveler. The
American Academ y of Family Physicians, 2003, 68(7): 1343-1350.
[10]
L. S.
Garcia.
Malaria. Clinical Laborator
y Medicine, 2010, 30(1):
93-129.
[11]
G. Dorsey, M. Gandhi, J. H. Oyugi
and P. J. Rosenthal. Difficul-
ties in the prevention, diagnosis, and treatment of imported ma-
laria. Archives of Internal Medicine, 2000, 160(16): 2505-
2510.
[12]
J. A. Martin, D. B. Mak. Changi
ng faces: A review of infectious
disease screening of refugees by
the Migrant Health Unit, Wes-
tern Australia in 2003 and 2004 , The Medical journal of A us tr ali a,
2006, 185(11-12): 607-610.
[13]
V. Johnston, J. M. Stockley, D. Dockrell,
et al
. Fever in returned
travellers presenting in the United Kingdom: Re commendations for
investigation and initial management. Journal of Infection, 2009,
59(1): 1-18.
[14]
E.
Bottieau
, J.
Clerinx
, W.
Schrooten
,
et
al
. Etiology and outcome
of fever after a stay in the tropics. Archives of Internal
M
edicine,
2006, 166(15): 1642-1648.
[15]
P
. A. Leggat. Assessment of febrile illness in the returned
traveller. Australian Family Physician, 2007, 36(5): 328-333.
[16]
H. C. Chung, J. T. Wang, H. Y. Sun,
et al
. Clinical experience of
17 cases of imported malaria at a Taiwan university hospital,
1999-2005. Journal of Microbiology Immunology and Infection,
2007, 40(3): 209-215.
[17]
C. H. Chuang. Current status of malaria in Taiwan from 1966 to
1990. The Kaohsiung Journal of Medical Sciences, 1991, 7(5): 23 3-
242.
[18]
J. S. Tang, C. L. Chen, W. C. Ko and C. C. Chuang. Imported
malaria in southern Taiwan from 1991 to 2002: A single hos-
pital’s experience. The Kaohsiung Journal of Medical Sciences,
2003, 19(8): 398-405.
[19]
H. C. Chung, J. T. Wang, H. Y. Sun,
et al
.
Clinical experience of
17 cases of i
mported malaria at a Taiwan university hospital,
1999-2005.
Journal of Microbiology Immunology and Infection,
2007,
40(3): 209-215.
[20]
C. T. Fang, S. C. Chang, H. L .Chang,
et al
. Imported malaria:
Successful treatment of 31 patient
s in the era of chloroquine
resistance. Journal of the Formosan Medical Association, 1999,
98(10): 683-687.
[21]
World Health Organization: Guidelines for the treatment of
Malaria, second edition, 2006.
http://www.who.int/malaria/publications/atoz/9789241547925/e
n/index.htm/
[22]
A. Dondorp, F. No sten, K. Stepniewska,
et al
. Artesunate versus
quinine for treatment of severe falciparum malaria: A random
trial. Lancet, 2005, 366: 717-725.
[23]
K. Yip. Malaria eradication: The Taiwan experience. Parassito-
logia, 2000, 42(1-2): 117-126.
[24]
C. T. Fang, H. L. Chang and W. C. Hsieh. Malaria eradication on
islands. Lancet, 2001, 357(9255): 560.
[25]
K. T. Chen, C. J. Chen, P. Y. Chang and D. L. Morse. A nosocomial
outbreak of malaria associated with contaminated catheters and
contrast medium of a computed tomographic scanner. Infection
Control and Hospital Epidemiology, 1999, 20(1): 22-25.
14 Cop
yright © 2012 Hanspub