 Asian Case Reports in Oncology亚洲肿瘤科病例研究, 2012, 1, 11-13 http://dx.doi.org/10.12677/acrpo.2012.12003 Published Online October 2012 (http://www.hanspub.org/journal/acrpo.html) A Case Report of the Round Hepatic Ligament Being as Contents of Linea Alba Associated with Gastric Cancer Pengfei Wa ng1, Bin Chen2, Z e ngrong Jia1, Shaoliang Han1* 1Department of General Surgery, The First Affiliated Hospital of Wenzhou Medical College, Wenzhou 2Department of Sonography, The First Affiliated Hospital of Wenzhou Medical College, Wenzhou Email: *slhan88@yahoo.com.cn Received: Jul. 4th, 2012; revised: Jul. 17th, 2012; accepted: Aug. 3rd, 2012 Abstract: A 70 year-old woman with chief complaint of an epigastric abdominal wall for more than 60 years, and dull pain in epigastria for 1 month. The general condition of this patient was good on physical examination, and patient was found with pale face and conjunctiva and negative yellow sclera. An abdominal soft mass sized in 6 cm × 4 cm, and was unable to push back abdominal cavity. Ultrasound showed that the echo of subcutaneous fascia was interrupted with a 9 mm long defect, and a mass about 53 mm × 20 mm × 39 mm with slightly strong echo was found superiorly, and bowel and omentum-like tissues seemed to connect with intra-abdominal cavity. Moreover, abdominal CT scan demonstrated that linea alba hernia. An irregular ulcer sized 4 cm × 3.5 cm was found by gastroscopy, and poorly-differentiated ade- nocarcinoma proven by biopsy. Furthermore, laboratory examination showed that hemoglobin was 73 g/L, and carci- noembryonic antigen (CEA) 3.0 ug/L. A exploratory laparotomy wad performed under epidural anesthesia, a soft, yel- lowish, sized 3 cm × 4 cm × 4 cm tumor was found in lineal alba, which connected with round hepatic ligament; the gastric cancer located at gastric antrum, about 5 cm × 4 cm, with serosal invasion and Borrmann type 3. Therefore, a radical distal gastrectomy and linea albs hernia repair were performed. The recovered smoothly and discharged healthy. Keywords: Linea Alba; Round Hepatic Ligament; Gastric Cancer 腹白线疝内容物为肝圆韧带并发胃癌一例 王鹏飞 1,陈 斌2,贾增荣 1,韩少良 1* 1温州医学院附属第一医院普外科,温州 2温州医学院附属第一医院超声科,温州 Email: *slhan88@yahoo.com.cn 收稿日期:2012 年7月4日;修回日期:2012年7月17 日;录用日期:2012年8月3日 摘 要:女性,70 岁,主诉上腹壁包块 60 余年,上腹部隐痛 1月余。查体:一般情况尚可,贫血貌,结膜苍 白(++),巩膜黄染(−)。上腹部正中可及一6 cm × 4 cm一包块,质软,不能回纳。腹部 B超检查示:上腹部腹 壁皮下深筋膜回声中断,有一个缺口约9 mm,其浅方可见一个53 mm × 20 mm × 39 mm 偏强回声团块,内见蠕 动的肠管及网膜样组织,通过此缺口与腹腔相通,提示腹白线疝。腹部 CT 扫描提示:上腹前壁中线处皮下脂 性团片影,考虑腹白线疝可能。胃镜检查:胃窦部见一个不规则隆起,大小约4 cm × 3.5 cm,表面溃烂,病理 示:低分化腺癌。实验室检查:血红蛋白(Hb)73 g/L,癌胚抗原(CEA)3.0 ug/L。在硬膜外麻醉下行剖腹探查:术 中见腹白线处有一个3 cm × 4 cm × 4 cm肿块,边界清,淡黄色,质软,与肝圆韧带顺序相连;肿瘤位于胃窦部 小弯侧后壁,Borromann3 型,约5 cm × 4 cm大小,穿透浆膜面,故行“根治性胃远端大部切除(D2+),腹白线 疝修补术”,术后恢复顺利,痊愈出院。 *通讯作者。 Copyright © 2012 Hanspub 11 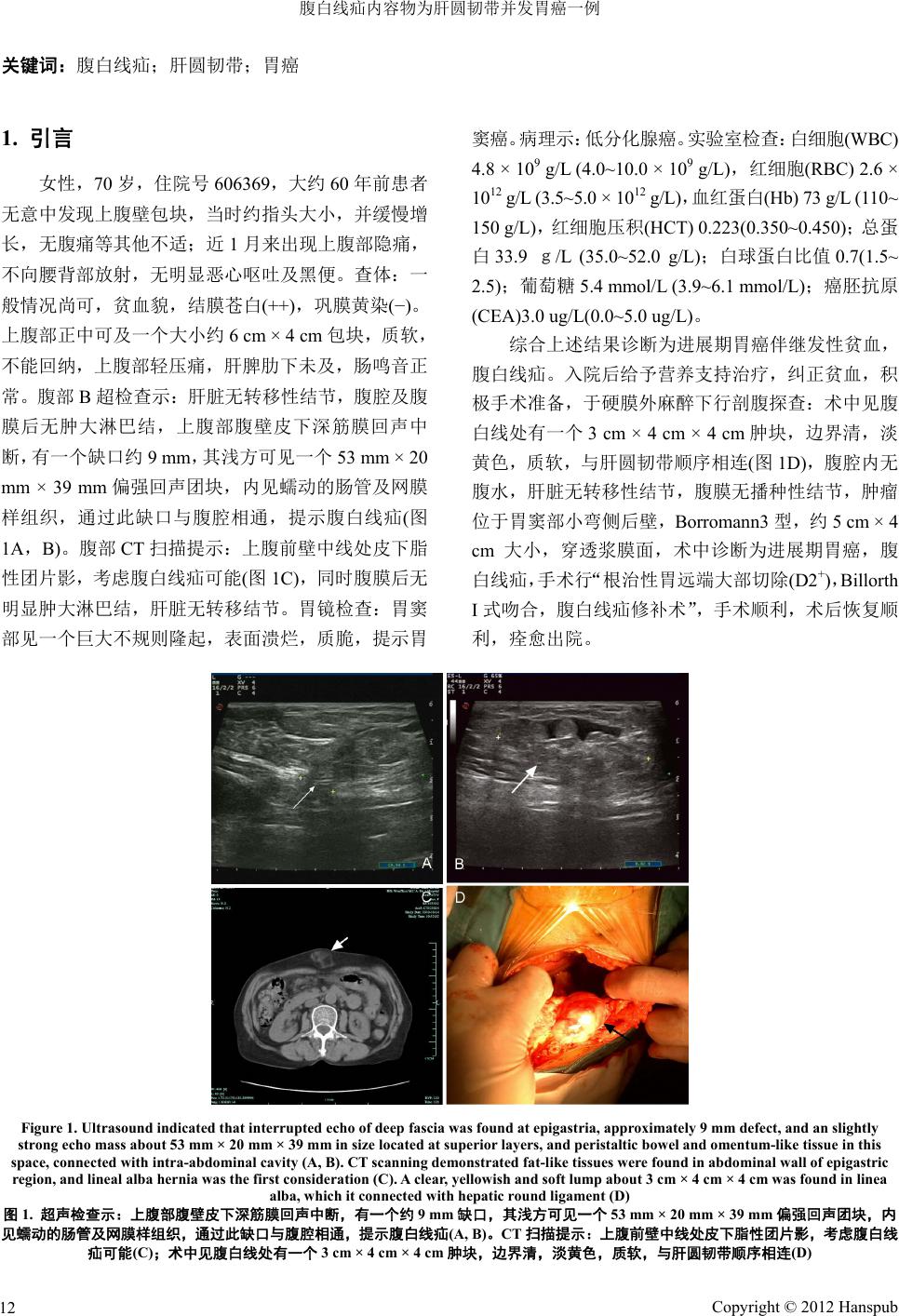 腹白线疝内容物为肝圆韧带并发胃癌一例 Copyright © 2012 Hanspub 12 关键词:腹白线疝;肝圆韧带;胃癌 1. 引言 窦癌。病理示:低分化腺癌。实验室检查:白细胞(WBC) 4.8 × 109 g/L (4.0~10.0 × 109 g/L),红细胞(RBC) 2.6 × 1012 g/L (3.5~5.0 × 1012 g/L),血红蛋白(Hb) 73 g/L (110~ 150 g/L),红细胞压积(HCT) 0.223(0.350~0.450);总 蛋 白33.9 g/L (35.0~52.0 g/L);白球蛋白比值0.7(1.5~ 2.5);葡萄糖 5.4 mmol/L (3.9~6.1 mmol/L);癌胚抗原 (CEA)3.0 ug/L(0.0~5.0 ug/L)。 女性,70 岁,住院号6 06369,大约 60 年前患者 无意中发现上腹壁包块,当时约指头大小,并缓慢增 长,无腹痛等其他不适;近1月来出现上腹部隐痛, 不向腰背部放射,无明显恶心呕吐及黑便。查体:一 般情况尚可,贫血貌,结膜苍白(++),巩膜黄染(−)。 上腹部正中可及一个大小约6 cm × 4 cm 包块,质软, 不能回纳,上腹部轻压痛,肝脾肋下未及,肠鸣音正 常。腹部 B超检查示:肝脏无转移性结节,腹腔及腹 膜后无肿大淋巴结,上腹部腹壁皮下深筋膜回声中 断,有一个缺口约 9 mm,其浅方可见一个53 mm × 20 mm × 39 mm偏强回声团块,内见蠕动的肠管及网膜 样组织,通过此缺口与腹腔相通,提示腹白线疝(图 1A,B)。腹部 CT 扫描提示:上腹前壁中线处皮下脂 性团片影,考虑腹白线疝可能(图1C),同时腹膜后无 明显肿大淋巴结,肝脏无转移结节。胃镜检查:胃窦 部见一个巨大不规则隆起,表面溃烂,质脆,提示胃 综合上述结果诊断为进展期胃癌伴继发性贫血, 腹白线疝。入院后给予营养支持治疗,纠正贫血,积 极手术准备,于硬膜外麻醉下行剖腹探查:术中见腹 白线处有一个3 cm × 4 cm × 4 cm肿块,边界清,淡 黄色,质软,与肝圆韧带顺序相连(图1D),腹腔内无 腹水,肝脏无转移性结节,腹膜无播种性结节,肿瘤 位于胃窦部小弯侧后壁,Borromann3 型,约 5 cm × 4 cm 大小,穿透浆膜面,术中 诊断为进 展期 胃癌, 腹 白线疝,手术行“根治性胃远端大部切除(D2+),Billorth I式吻合,腹白线疝修补术”,手术顺利,术后恢复顺 利,痊愈出院。 Figure 1. Ultrasound indicated that interrupted echo of deep fascia was found at epigastria, approximately 9 mm defect, and an slightly strong echo mass about 53 mm × 20 mm × 39 mm in size located at superior layers, and peristaltic bowel and omentum-like tissue in this space, connected with intra-abdominal cavity (A, B). CT scanning demonstrated fat-like tissues were found in abdominal wall of epigastric region, and lineal alba hernia was the first consideration (C). A clear, yellowish and soft lump about 3 cm × 4 cm × 4 cm was found in linea alba, which it connected with hepatic round ligament (D) 图1. 超声检查示:上腹部腹壁皮下深筋膜回声中断,有一个约 9 mm缺口,其浅方可见一个 53 mm × 20 mm × 39 mm偏强回声团块,内 见蠕动的肠管及网膜样组织,通过此缺口与腹腔相通,提示腹白线疝(A, B)。CT 扫描提示:上腹前壁中线处皮下脂性团片影,考虑腹白线 疝可能(C);术中见腹白线处有一个 3 cm × 4 cm × 4 cm肿块,边界清,淡黄色,质软,与肝圆韧带顺序相连(D)  腹白线疝内容物为肝圆韧带并发胃癌一例 2. 讨论 白线疝属临床上少见腹内疝,它可发生于腹壁正 中线(即腹白线)的不同部位,但绝大数位于脐上腹白 线[1]。腹白线的腱纤维均为斜行交叉,这一结构可使 白线作出形态和大小改变以适应躯体活动或腹壁活 动的变化。但当腹内压力增高(如慢性咳嗽、慢性便秘、 排尿困难、腹水、妊娠及举重等),同时腹壁强度降低 (如腹白线发育不全、手术切口愈合不良、老年、久病 及肥胖所致肌萎缩等)时,就有可能撕裂交叉的腱纤 维,从而逐渐形成白线疝[1-3]。如果仅有膜外脂肪组织 从此间隙中疝出,此时疝内容物为脂肪组织,无疝囊 (无疝囊型)。随着病情进一步发展,突出的腹膜外脂 肪可把腹膜向外牵出形成疝囊(有疝囊型),进而腹内 组织(通常是大网膜,少数可是肝圆韧带、肠管(Richter 疝)、扩张的腹腔内血管和肝脏等)通过疝颈进入疝囊 [1,3,4]。本例患者从儿童时期即发 现前腹壁肿块 ,考虑 与腹白线先天性薄弱有关。 作者查阅 1989 年以后中文文献及1977 年以后 Medline 文献后仅发现2例疝内容物为肝圆韧带的腹 白线疝报道,国内外各1例[2,3]。由于本病早期腹块较 小,仅表现为上消化道症状如上腹钝痛、烧灼痛、或 痉挛性疼痛、腹胀、消化不良、恶心和呕吐等,其典 型病例是饱餐后站立时加重或在用力时上腹痛。故常 被漏诊或误诊为消化道疾病(如胆道疾病、溃疡病、慢 性胰腺炎等)。因此,凡是有上述症状的患者,应仔细 检查有无微小有压痛的肿块或白线上的缺损。倘若腹 白线肿块可以复位,应考虑到本病。另外,白线疝需 要与生长缓慢的脂肪瘤、纤维瘤、神经纤维瘤及低度 恶性的硬纤维瘤等前腹壁肿瘤相鉴别[1,2]。不过,像本 例同时并发胃癌的腹白线疝病例,尚需与腹腔内癌瘤 的脐部转移(Mary Joseph sister结节)和术后切口肿瘤 种植转移相鉴别[5]。 多数认为凡临床症状明显或直径大于0.5 cm的 白线疝,均应早期手术治疗,避免病情加重。手术多 采用纵形切口,切开皮下组织后仔细分离脱出的脂肪 组织,充分显露白线,然后处理疝囊:1) 无疝囊型: 将突出的腹膜前脂肪稍向外牵拉后于根部结扎切断, 使脂肪回缩至白线后方,而后修补白线缺损;2) 有疝 囊型:切开疝囊、还纳内容物,疝囊颈部高位结扎、 切除疝囊,再修补白线缺损;3) 如果白线间隙(疝环) 较大,应采用重叠缝合腹白线或应用各种补片进行无 张力修补,以加强腹壁、防止复发;4) 也可采用腹腔 镜下疝修补[2-6]。本例因为腹白线疝较小,故仅切除疝 出腹壁的多余肝圆韧带,直接将两侧的腹直肌前后鞘 间断缝合修补,术后痊愈出院。 参考文献 (References) [1] B. Lang, H. Lau and F. Lee. Epigastric hernia and its etiology. Hernia, 2002, 6(3): 148-150. [2] M. Jacob, R. Saif, G. Sen, et al. Laparoscopic repair of a rare case of falciform ligament herniation. Journal of Laparoendo- scopic & Advanced Surgical Techniques A, 2010, 20(9): 767- 769. [3] N. V. Turkina, S. M. Pudiakov, A. A. Babkov, et al. Strangulation of the round hepatic ligament in white-line abdominal hernia. Vestnic Khirurgii Imeni I. I. Grekova, 1990, 145(11): 50-51. [4] 李有, 李润海. 疝内容物为肝圆韧带的白线疝一例报告[J]. 腹部外科, 2006, 19(4): 246. [5] P. Y. Marcy, O. Hericord, A. Italiano, et al. Linea alba tumoral (sarcomatous) hernia. JBR-BTR, 2006, 89(2): 103. [6] 陈其龙, 牟一平, 周育成等. 多点悬吊法腹腔镜修补白线疝 一例[J]. 浙江大学学报(医学版), 2011, 40(5): 573-574. Copyright © 2012 Hanspub 13 |