Hans Journal of Ophthalmology
Vol.
09
No.
03
(
2020
), Article ID:
37473
,
4
pages
10.12677/HJO.2020.93026
双眼睑结膜结核性肉芽肿一例
文瑾1*,严梦南2,3
1甘肃省人民医院,甘肃 兰州
2甘肃中医药大学,甘肃 兰州
3甘肃中医药大学附属兰州华厦眼科医院,甘肃 兰州

收稿日期:2020年8月14日;录用日期:2020年8月28日;发布日期:2020年9月4日

摘要
结核杆菌主要感染部位为肺部,眼结核发病率较低,为1.4%~5.74%,眼部因脉络膜氧含量较高,毛细血管丰富且血流缓慢,结核杆菌易滞留于此,最常见的临床表现是葡萄膜炎,原发性结膜和眼睑结核性肉芽肿很少发生。本案例中,患者主因“双眼睑红肿、流泪、视物模糊2月”以“双眼睑板腺囊肿”收住,术后病理示:考虑结核性肉芽肿。临床工作中,医生应加强对眼结核的认识,避免误诊误治,延误患者病情。
关键词
眼结核,结核肉芽肿

Tuberculous Granuloma of Conjunctiva in Both Eyes: A Case Report
Jin Wen1*, Mengnan Yan2,3
1Gansu Provincial People’s Hospital, Lanzhou Gansu
2Gansu University of Traditional Chinese Medicine, Lanzhou Gansu
3Lanzhou Ophthalmology Center Affiliated to Gansu University of Traditional Chinese Medicine, Lanzhou Gansu
Received: Aug. 14th, 2020; accepted: Aug. 28th, 2020; published: Sep. 4th, 2020

ABSTRACT
The main infection area of Mycobacterium tuberculosis is lung, and the incidence rate of ocular tuberculosis is low. It is 1.4% - 5.74%. The ocular area is high in choroidal oxygen content, abundant in capillary and slow in blood flow. Tuberculosis is easy to stay here. The most common clinical manifestation is uveitis, primary conjunctiva and nucleate granuloma of eyelid. In this case, the patient received “meibomian gland cyst” because of “redness and swelling of both eyelids, tears and blurred vision for 2 months”. Postoperative pathology showed that tuberculous granuloma was considered. In clinical work, doctors should strengthen the understanding of ocular tuberculosis, avoid misdiagnosis and mistreatment, and delay the patient’s condition.
Keywords:Ocular Tuberculosis, Tuberculous Granuloma

Copyright © 2020 by author(s) and Hans Publishers Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY 4.0).
http://creativecommons.org/licenses/by/4.0/


1. 引言
结核病是一种传染性疾病,主要好发部位为肺部,眼结核发病率相对较低。在眼部,结核分枝杆菌倾向于在区域氧含量较高的脉络膜和睫状体生长,结膜结核较少见,且眼结核的诊断金标准是活检,取材不易,诊断困难。结核病是一个严重的全球健康问题,已成为世界范围内导致死亡的主要原因之一,因此正确诊治结核病至关重要 [1]。
2. 临床资料
患者男性,23岁,既往体健,主因“双眼睑红肿、流泪、视物模糊2月”于2019年1月9日就诊于甘肃省人民医院。查体:神志清,精神可,生命体征平稳。眼科专科检查:矫正视力:右眼0.6,左眼1.0;眼压:右眼15 mmHg,左眼18 mmHg;右眼眼睑肿胀,睁眼困难,睑板腺口脂溢,充血(++++),上下睑结膜多处局部红色隆起,大小不等,最大者约为8 × 4 mm,质软,无明显压痛,边界清晰,不能活动,可见数个黄白色结膜结石,余未见明显异常(如图1所示)。左眼大致同右眼。抗核抗体(IgM):阳性;抗核抗体(IgG):阳性;胸部X片:未见明显异常。2019年1月10日在局麻下行“双眼睑板腺病损切除术”,术中切开并刮除多个隆起组织,共清理上下睑睑板腺囊肿12余处,局部肉芽组织切除送病检。病理诊断:慢性肉芽肿性炎,高度考虑:1) 结核感染;2) 麦粒肿、皮脂腺或睑板腺囊肿破裂溢出或霉菌感染所致(如图2所示)。术后局部给予典必殊眼膏点双眼4次/天,术后三日出院,嘱其结核病医院进一步详查就诊。一周后复查,查体:矫正视力:右眼0.8,左眼1.0,结膜手术切口愈合良好,一月、三月后复查,未见结膜结核肉芽肿复发,患者未诉全身肺结核症状。本研究已获得患者的知情同意。
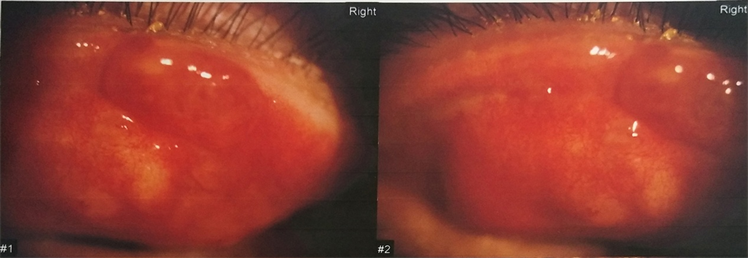
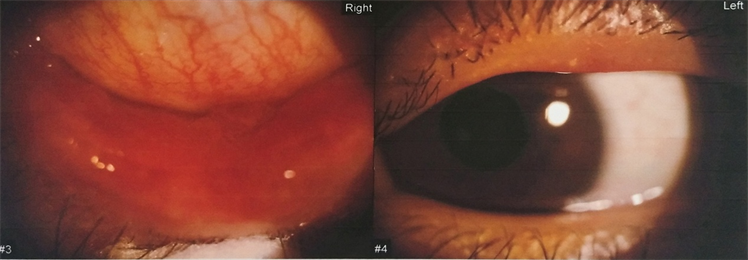
Figure 1. Preoperative anterior segment photography of this patient: palpebral conjunctiva and bulbar conjunctiva are hyperemia, several conjunctival proliferators, boundaries clear, no purulent secretions were found on the surface
图1. 患者术前眼前段照相:睑结膜、球结膜充血,数个结膜增生物,边界清晰,表面未见脓性分泌物)
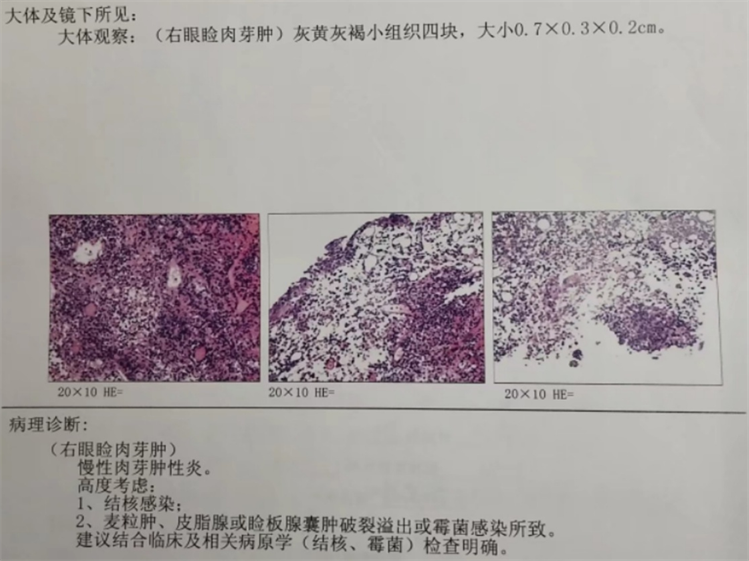
Figure 2. Postoperative pathological diagnosis of the patient: tuberculous granuloma was considered
图2. 患者术后病理诊断:考虑结核性肉芽肿
3. 讨论
结核病发病率和流行率最近呈下降趋势,但世卫组织估计,2010年有880万例结核病病例,死亡145万人,其中中国、印度和非洲是新发和复发病例最多的国家 [2]。主要感染部位为肺部,眼结核发病率较低,为1.4%~5.74%,在HIV患者中,发病率可能更高,从2.8%~11.4%不等 [3]。
本次诊治过程中,患者以“多发性睑板腺囊肿”收住,患者无全身结核病的典型症状,如:低烧、乏力、盗汗等,否认既往结核感染,否认结核病接触史,胸部X片未见明显异常,且眼部因脉络膜氧含量较高,毛细血管丰富且血流缓慢,结核杆菌易滞留于此,最常见的临床表现是葡萄膜炎,原发性结膜和眼睑结核性肉芽肿很少发生 [4],因此患者入院诊断时没有考虑到睑结膜结核性肉芽肿的可能性,术后病理检查才发现结核杆菌感染,修正诊断为原发性结膜结核。诊断眼结核的金标准是从眼组织或玻璃体中培养出结核杆菌,然而,在许多情况下,获得眼标本的风险是不可接受的 [5],且标本量少,结核杆菌培养要求高、时间较长,培养结果阳性率不高。本病例中,患者结核性肉芽肿在眼表,手术切除方便,标本容易获取,才得以明确诊断,没有造成误诊。因此可疑结核感染的患者,可先行治疗实验 [6],即对可疑结核感染的患者接受标准的抗结核治疗,几乎所有患者在4周后开始病情缓解、症状改善,才给予明确诊断。
目前还没有对眼结核的诊断方法达成共识,建议的临床方法包括首先识别提示性的临床症状,如:广泛性粘连、视网膜血管炎、多灶性脉络膜炎和血清型脉络膜炎 [7],随后采用阶梯式方法确认诊断:在出现提示性临床症状和排除其他病因后,患者接受结核病免疫试验(TST或IgRA)和胸部X光检查。根据检查结果,病人最终可以分为以下几类:明确的眼内结核(其中微生物或其DNA可以在眼内液体/组织中复制,这可能暗示有活动性或以前的结核感染);假定的眼内结核(在支持性试验阳性,经验性抗结核治疗有良好疗效);不太可能的眼内结核(检查结果不支持结核) [8]。
眼睛感染结核病是一种严重的疾病,任何诊断和治疗的延误都会导致失明。一位64岁的病人,被诊断为肺结核的四周内,左眼视力迅速恶化,最终失明 [9]。因此临床医师在诊疗过程中,应考虑到眼结核的可能性,避免造成漏诊误诊,贻误患者病情,及早开始标准抗结核治疗,挽救患者的视力。
文章引用
文 瑾,严梦南. 双眼睑结膜结核性肉芽肿一例
Tuberculous Granuloma of Conjunctiva in Both Eyes: A Case Report[J]. 眼科学, 2020, 09(03): 197-200. https://doi.org/10.12677/HJO.2020.93026
参考文献
- 1. (2015) Global Tuberculosis Report 2015. World Health Organization.
- 2. Behera, D. (2012) Global Tuberculosis Control 2011, WHO Report 2011. Indian Journal of Medical Research.
- 3. Kestelyn, P.G. and Cunningham, E.T. (2001) HIV/AIDS and Blindness. Bulletin of the World Health Organization, 79, 208-213.
- 4. Sharma, A., Thapa, B. and Lavaju, P. (2011) Ocular Tuberculosis: An Update. Nepalese Journal of Ophthalmology: A Biannual Peer-Reviewed Academic Journal of the Nepal Ophthalmic Society: NEPJOPH, 3, 52.
https://doi.org/10.3126/nepjoph.v3i1.4280 - 5. Yeh, S., Sen, H.N., Colyer, M., et al. (2012) Update on Ocular Tuberculosis. Current Opinion in Ophthalmology, 23, 551-556.
https://doi.org/10.1097/ICU.0b013e328358ba01 - 6. Ramam, M., Trilokraj, T., Yashpal, M., et al. (2007) What Is the Appropriate Duration of a Therapeutic Trial in Cutaneous Tuberculosis? Further Observations. Indian Journal of Dermatology Venereology & Leprology, 73, 243.
https://doi.org/10.4103/0378-6323.32890 - 7. Tognon, M.S., Fiscon, M., Mirabelli, P., et al. (2014) Tuberculosis of the Eye in Italy: A Forgotten Extrapulmonary Localization. Infection, 42, 335-342.
https://doi.org/10.1007/s15010-013-0554-4 - 8. Ang, M., Vasconcelossantos, D.V., Sharma, K., et al. (2016) Diagnosis of Ocular Tuberculosis. Ocular Immunology & Inflammation, 26, 1-9.
https://doi.org/10.1080/09273948.2016.1178304 - 9. Lim, C.W. and Chong, M.S. (2012) Ocular Tuberculosis—A Blinding Eye Infection. International Eye Science.