 Asian Case Reports in Surgery 亚洲外科手术病例研究, 2012, 1, 1-4 http://dx.doi.org/10.12677/acrs.2012.11001 Published Online June 2012 (http://www.hanspub.org/journal/acrs) Advances in Application of CBCT in Diagnosis and Treatment Designing of Mandible Fracture* Renfa Lai#, Qingtong Zhao, Shan Shen The Medical Centre of Stomatology, The 1st Affiliated Hospital of Jinan University, Guangzhou Email: #Prof.Dr.Lai@163.com Received: May 4th, 2012; revised: May 18th, 2012; accepted: May 28th, 2012 Abstract: Purpose: This paper is to illustrate and discuss the importance of cone beam computed tomography for ac- curate diagnose of mandible fracture and for the guidance of the operation designing. Method: A case of maxillofacial trauma was used for this report. A 38-year-old male patient was referred to Oral and Maxillofacial Department with a history of maxillofacial trauma. The history of patient revealed a traumatic injury on his face because worksite acci- dence. The patient as initially examined and diagnosed mandible fractures by a 2D panoramic film, but there isn’t any information about the displacement of the fracture ends and we don’t know the 3D structure about fracture ends. Therefore the 3D (CBCT) was performed. Results: Cone beam computed tomography (CBCT) images can offer an accurate diagnosis; it can show the displacement of the fracture end, it can also give the surgeon a useful guidance for the operation process. Conclusion: CBCT is a useful tool for making an accurate diagnosis of maxillofacial trauma and can guide the operation. Keywords: Mandible; Fracture; Displacement; CBCT; Operation 利用 CBCT 诊断及指导手术治疗下颌骨骨折* 赖仁发#,赵清桐,沈 山 暨南大学附属第一医院,口腔医疗中心,广州 Email: #Prof.Dr.Lai@163.com 收稿日期:2012 年5月4日;修回日期:2012 年5月18 日;录用日期:2012年5月28 日 摘 要:目的:探讨 CBCT 对诊断及指导外科手术治疗下颌骨骨折的临床意义。方法:通过临床典型病例,分 析下颌骨骨折发生时作曲面断层片检查易造成漏诊/误诊,CBCT 能从冠状位、轴向位、矢状位等不同的角度及 方向观察颌骨骨折端。结果:CBCT 能清晰了解骨折线走向及断端与骨折碎片的移位情况,能指导外科手术治疗 骨折的复位与作内固定。CBCT三维重建有益颌面外科制定手术计划。 关键词:下颌骨;骨折;移位;CBCT;治疗 1. 引言 在颌面部外伤中,下颌骨因为其突出的位置而致 发生骨折的机率较高,常规的曲面断层片检查时有漏 诊或误诊现象,因此而导致的延误治疗将影响患者的 颌面形态和功能,还将引起医疗纠纷,随 CBCT(cone beam computerized tomography, CBCT)技术在口腔颌 面部的临床应用,本文结合我们的临床病例应用体 会,报告分析锥形束 CT 在诊断下颌骨骨折及指导外 科手术治疗时的临床作用。 2. 临床病例 *基金项目:广东省科技产业技术研究与开发项目(编号:2011B 080701053)。#通讯作者。 患者张某,男,38岁,因为工伤事故外伤送来就 Copyright © 2012 Hanspub 1 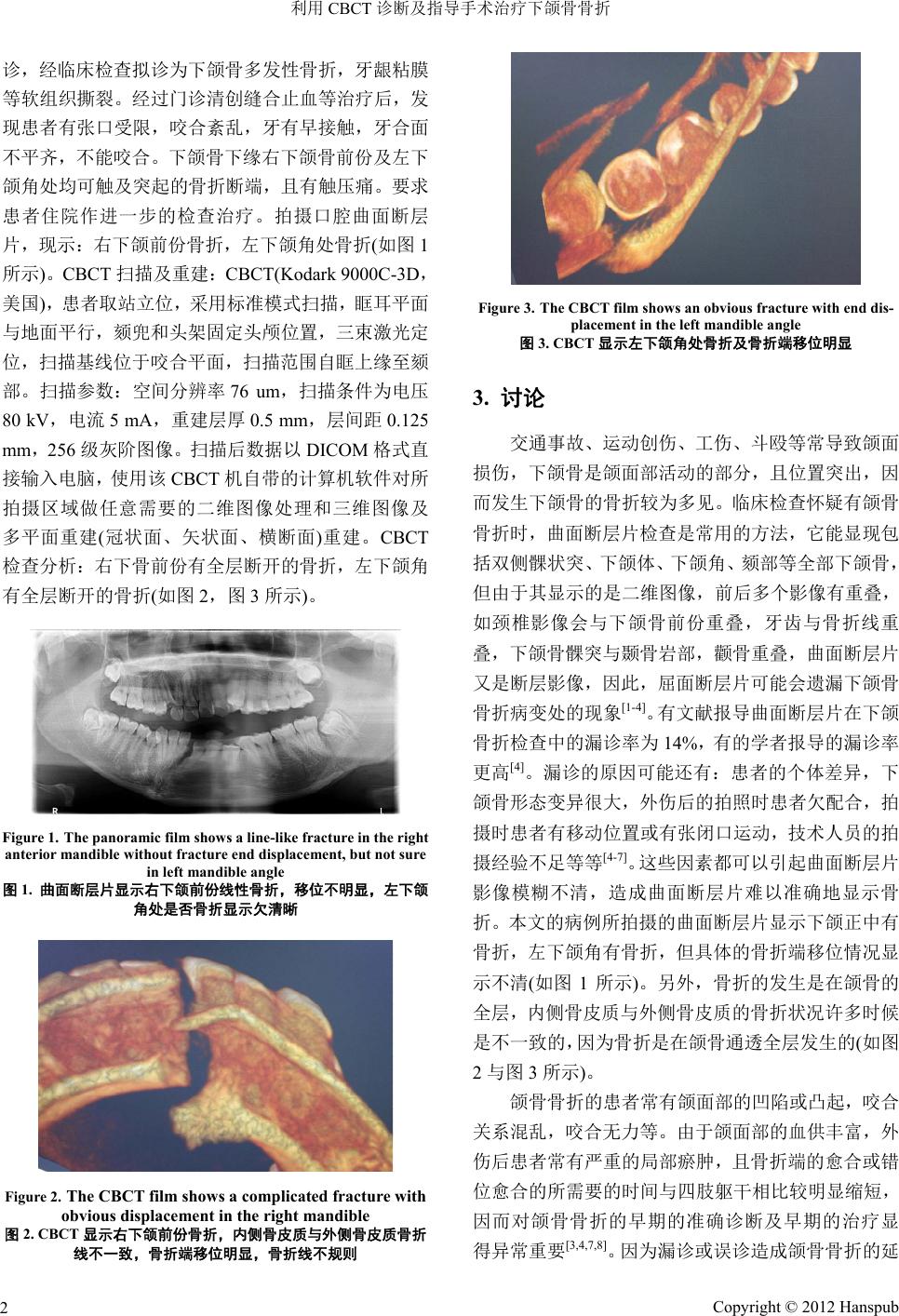 利用 CBCT 诊断及指导手术治疗下颌骨骨折 诊,经临床检查拟诊为下颌骨多发性骨折,牙龈粘膜 等软组织撕裂。经过门诊清创缝合止血等治疗后,发 现患者有张口受限,咬合紊乱,牙有早接触,牙合面 不平齐,不能咬合。下颌骨下缘右下颌骨前份及左下 颌角处均可触及突起的骨折断端,且有触压痛。要求 患者住院作进一步的检查治疗。拍摄口腔曲面断层 片,现示:右下颌前份骨折,左下颌角处骨折(如图 1 所示)。CBCT 扫描及重建:CBCT(Kodark 9000C-3D, 美国),患者取站立位,采用标准模式扫描,眶耳平面 与地面平行,颏兜和头架固定头颅位置,三束激光定 位,扫描基线位于咬合平面,扫描范围自眶上缘至颏 部。扫描参数:空间分辨率76 um,扫描条件为电压 80 kV,电流 5 mA,重建层厚 0.5 mm,层间距 0.125 mm,256 级灰阶图像。扫描后数据以 DICOM 格式直 接输入电脑,使用该CBCT机自带的计算机软件对所 拍摄区域做任意需要的二维图像处理和三维图像及 多平面重建(冠状面、矢状面、横断面)重建。CBCT 检查分析:右下骨前份有全层断开的骨折,左下颌角 有全层断开的骨折(如图 2,图3所示)。 Figure 1. The panoramic film shows a line-like fracture in the right anterior mandible without fracture end displacement, but not sure in left mandible angle 图1. 曲面断层片显示右下颌前份线性骨折,移位不明显,左下颌 角处是否骨折显示欠清晰 Figure 2. The CBCT film shows a complicated fracture with obvious displacement in the right mandible 图2. CBCT显示右下颌前份骨折,内侧骨皮质与外侧骨皮质骨折 线不一致,骨折端移位明显,骨折线不规则 Figure 3. The CBCT film shows an obvious fracture with end dis- placement in the left mandible angle 图3. CBCT显示左下颌角处骨折及骨折端移位明显 3. 讨论 交通事故、运动创伤、工伤、斗殴等常导致颌面 损伤,下颌骨是颌面部活动的部分,且位置突出,因 而发生下颌骨的骨折较为多见。临床检查怀疑有颌骨 骨折时,曲面断层片检查是常用的方法,它能显现包 括双侧髁状突、下颌体、下颌角、颏部等全部下颌骨, 但由于其显示的是二维图像,前后多个影像有重叠, 如颈椎影像会与下颌骨前份重叠,牙齿与骨折线重 叠,下颌骨髁突与颞骨岩部,颧骨重叠,曲面断层片 又是断层影像,因此,屈面断层片可能会遗漏下颌骨 骨折病变处的现象[1-4]。有文献报导曲面断层片在下颌 骨折检查中的漏诊率为14%,有的学者报导的漏诊率 更高[4]。漏诊的原因可能还有:患者的个体差异,下 颌骨形态变异很大,外伤后的拍照时患者欠配合,拍 摄时患者有移动位置或有张闭口运动,技术人员的拍 摄经验不足等等[4-7]。这些因素都可以引起曲面断层片 影像模糊不清,造成曲面断层片难以准确地显示骨 折。本文的病例所拍摄的曲面断层片显示下颌正中有 骨折,左下颌角有骨折,但具体的骨折端移位情况显 示不清(如图 1所示)。另外,骨折的发生是在颌骨的 全层,内侧骨皮质与外侧骨皮质的骨折状况许多时候 是不一致的,因为骨折是在颌骨通透全层发生的(如图 2与图 3所示)。 颌骨骨折的患者常有颌面部的凹陷或凸起,咬合 关系混乱,咬合无力等。由于颌面部的血供丰富,外 伤后患者常有严重的局部瘀肿,且骨折端的愈合或错 位愈合的所需要的时间与四肢躯干相比较明显缩短, 因而对颌骨骨折的早期的准确诊断及早期的治疗显 得异常重要[3,4,7,8]。因为漏诊或误诊造成颌骨骨折的延 Copyright © 2012 Hanspub 2 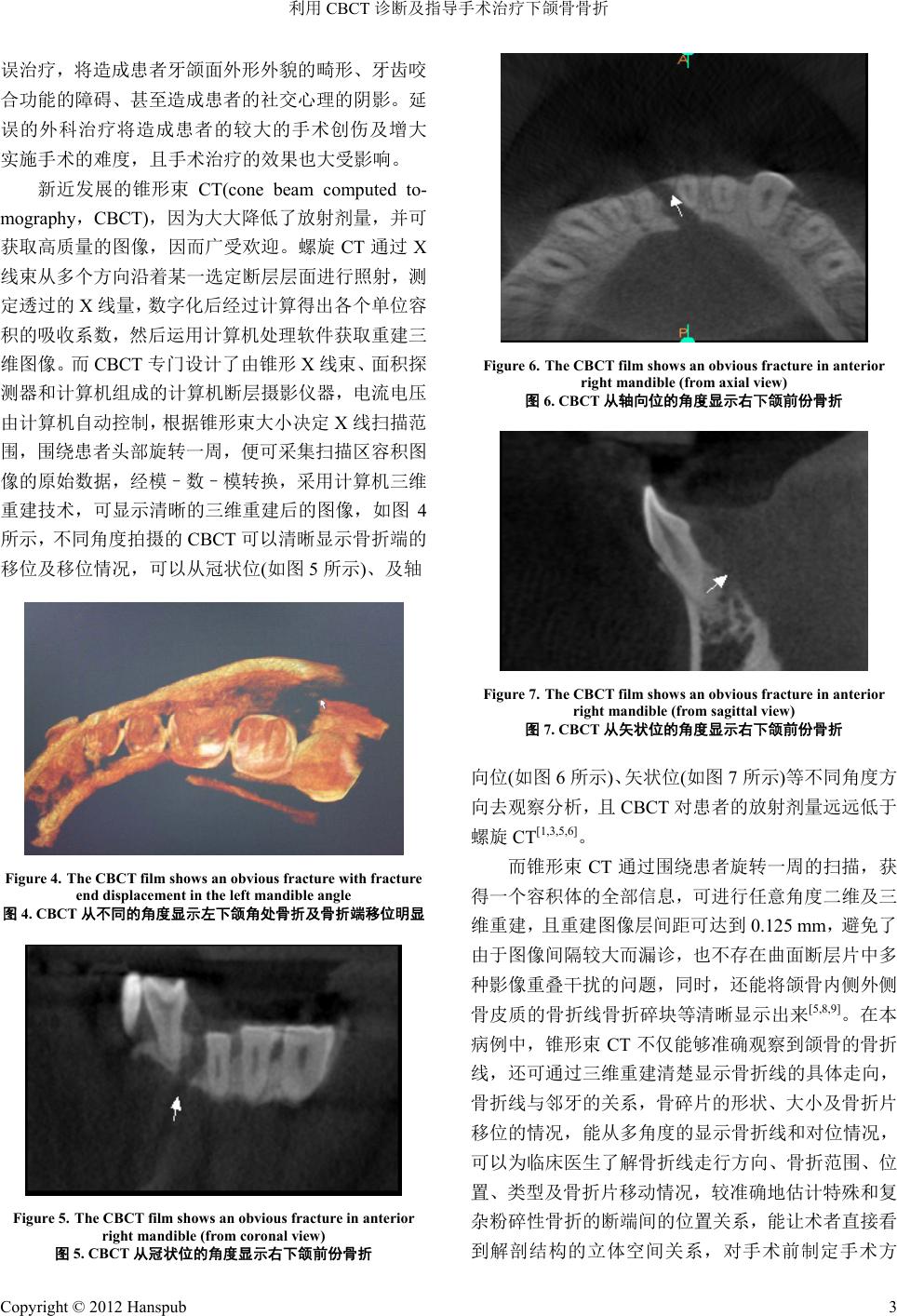 利用 CBCT 诊断及指导手术治疗下颌骨骨折 误治疗,将造成患者牙颌面外形外貌的畸形、牙齿咬 合功能的障碍、甚至造成患者的社交心理的阴影。延 误的外科治疗将造成患者的较大的手术创伤及增大 实施手术的难度,且手术治疗的效果也大受影响。 新近发展的锥形束 CT(cone beam computed to- mography,CBCT),因为大大降低了放射剂量,并可 获取高质量的图像,因而广受欢迎。螺旋CT 通过X 线束从多个方向沿着某一选定断层层面进行照射,测 定透过的 X线量,数字化后经过计算得出各个单位容 积的吸收系数,然后运用计算机处理软件获取重建三 维图像。而CBCT 专门设计了由锥形 X线束、面积探 测器和计算机组成的计算机断层摄影仪器,电流电压 由计算机自动控制,根据锥形束大小决定 X线扫描范 围,围绕患者头部旋转一周,便可采集扫描区容积图 像的原始数据,经模–数–模转换,采用计算机三维 重建技术,可显示清晰的三维重建后的图像,如图 4 所示,不同角度拍摄的CBCT 可以清晰显示骨折端的 移位及移位情况,可以从冠状位(如图 5所示)、及轴 Figure 4. The CBCT film shows an obvious fracture with fracture end displacement in the left mandible angle 图4. CBCT从不同的角度显示左下颌角处骨折及骨折端移位明显 Figure 5. The CBCT film shows an obvious fracture in anterior right mandible (from coronal view) 图5. CBCT从冠状位的角度显示右下颌前份骨折 Figure 6. The CBCT film shows an obvious fracture in anterior right mandible (from axial view) 图6. CBCT从轴向位的角度显示右下颌前份骨折 Figure 7. The CBCT film shows an obvious fracture in anterior right mandible (from sagittal view) 图7. CBCT从矢状位的角度显示右下颌前份骨折 向位(如图 6所示)、矢状位(如图7所示)等不同角度方 向去观察分析,且CBCT对患者的放射剂量远远低于 螺旋 CT[1,3,5,6]。 而锥形束 CT 通过围绕患者旋转一周的扫描,获 得一个容积体的全部信息,可进行任意角度二维及三 维重建,且重建图像层间距可达到 0.125 mm,避免了 由于图像间隔较大而漏诊,也不存在曲面断层片中多 种影像重叠干扰的问题,同时,还能将颌骨内侧外侧 骨皮质的骨折线骨折碎块等清晰显示出来[5,8,9]。在本 病例中,锥形束 CT 不仅能够准确观察到颌骨的骨折 线,还可通过三维重建清楚显示骨折线的具体走向, 骨折线与邻牙的关系,骨碎片的形状、大小及骨折片 移位的情况,能从多角度的显示骨折线和对位情况, 可以为临床医生了解骨折线走行方向、骨折范围、位 置、类型及骨折片移动情况,较准确地估计特殊和复 杂粉碎性骨折的断端间的位置关系,能让术者直接看 到解剖结构的立体空间关系,对手术前制定手术方 Copyright © 2012 Hanspub 3  利用 CBCT 诊断及指导手术治疗下颌骨骨折 Copyright © 2012 Hanspub 4 层片检查仍然是诊断下颌骨骨折常用 的检 参考文献 (References) et al. A comparative evaluation son, A. Lokeh, C. I. Benjamin, et al. Contribution of M. Otonari-Yamamoto, T. Sano, et al. Cone-beam CT l. Accuracy of of optimal condylar posi- . Bjornland. Image-guided puncture technique for low, M. Ivanovic. Comparative dosimetry of dental ndication for ationship between 案、手术进路、复位固定的方法及术后观察疗效都极 有帮助[10,11]。 尽管曲面断 查方法,但因为其存在漏诊/误诊的可能性,特别 是在髁突或颏部骨折时,漏诊/误诊的风险更大。因此, 临床上对于可疑的颌骨骨折,特别是怀疑下颌骨髁状 突或颌骨颏部骨折时,需要进一步作 CBCT 检查,另 外对于颌骨复杂的骨折,需要了解骨折碎片、骨折的 移位走向时,也需要行 CBCT 检查,以获得有益的信 息。CBCT 除了能确定骨折部位,骨折走向、骨折碎 片大小外,其多角度的三维重建图像可清晰显示骨折 段移位的详细情况,为临床制定合理的手术进路、手 术复位骨折端及骨折片的方法、坚固内固定方案等提 供帮助,在颌面外科临床工作中有着广泛的应用前景。 [1] X. Liang, R. Jacobs, B. Hassan, of Cone Beam Computed Tomography (CBCT) and Multi-Slice CT (MSCT) Part I. On subjective image quality. European Jour- nal of Radiology, 2010, 75(2): 265-269. [2] T. Kagawa, F. Fukunari, T. Shiraishi, et al. Development of a simple image viewer designed for small X-ray field CT equip- ment 3DX. Oral Radiology, 2006, 22(2): 47-51. [3] R. Lai, H. Zou, W. Kong, et al. The applied anatomic site study of the palatal anchorage implants using cone beam computed tomography. International Journal of Oral Science, 2010, 2(2): 98-104. [4] I. F. Wil conventional axial computed tomography (nonhelical), in con- junction with panoramic tomography (zonography), in evaluat- ing mandibular fractures. Annals of Plastic Surgery, 2000, 45(4): 415-421. [5] A. Yajima, (CBThrone) applied to dentomaxillofacial region. The Bulletin of Tokyo Dental College, 2006, 47(3): 133-141. [6] O. B. Honey, W. C. Scarfe, M. J. Hilgers, et a cone-beam computed tomography imaging of the tmporoman- dibular joint: Comparisons with panoramic radiology and linear tomography. American Journal of Orthodontics and Dentofacial Orthopedics, 2007, 132(4): 429-438. [7] K. Ikeda, A. Kawamura. Assessment tion with limited cone-beam computed tomography. American Journal of Orthodontics an d Dentofacial Orthop edics, 2009, 1 35 ( 4) : 495 -501. [8] K. Honda, T the superior temporomandibular joint space: Value of cone beam computed tomography (CBCT). Oral Surgery, Oral Medicine, Oral Pathology , Oral Radiology and Endodontology, 2006, 102(3): 281-286. [9] J. B. Lud CBCT devices and 64-slice CT for oral and maxillofacial radi- ology. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radi- ology and Endodontology, 2008, 106(1): 106-114. [10] J. Klatt, M. Heiland, M. Blessmann, et al. Clinical i intraoperative 3D imaging during open reduction of fractures of the neck and head of the mandibular condyle. Journal of Cranio- Maxillofacial Surgery, 2011, 39(4): 244-248. [11] N. Kijima, K. Honda, Y. Kuroki, et al. Rel patient characteristics, mandibular head morphology and thick- ness of the roof of the glenoid fossa in symptomatic temporo- mandibular joints. Dentomaxillofacial Radiology, 2007, 36(5): 277-281. |