Medical Diagnosis
Vol.
10
No.
04
(
2020
), Article ID:
39556
,
9
pages
10.12677/MD.2020.104038
腹股沟入路与Stoppa入路在应用3D打印导板治疗髋臼骨折的对比研究
邵莉剑
横店文荣医院骨科,浙江 金华

收稿日期:2020年11月20日;录用日期:2020年12月23日;发布日期:2020年12月30日

摘要
目的:比较腹股沟入路与Stoppa入路在应用3D打印导板治疗髋臼骨折的效果,寻找最佳的手术入路方案。方法:本研究选取自2012年1月~2019年1月入我院创伤外科的142例患者,所有患者均采用术前3D打印技术模拟患者髋臼骨折的损伤类型,术前根据骨折的类型对钢板进行预先塑形或者直接定制个体化钢板,根据手术入路随机分成2组,其中腹股沟入路组68例,男性46例,女性22例;Stoppa入路组74例,男性51例,女性23例。收集患者的CT + 三维重建资料和髂血管CTA的数据,以DICOM形式保存,导入Mimic软件中,进行软件处理,对髋臼骨折进行还原。同时采用3ds Max 2013软件,对骨折的复位,螺钉的位置和大小进行设计。统计并记录手术显露时间、切口长度、术中出血量;利用Matta影像学评分评价髋臼骨折复位质量,根据髋关节Postel评分评价髋关节功能。结果:2组患者一般基准资料比较无统计学差异(P > 0.05)。Mimic软件模拟骨盆髋臼骨折,并且利用Mimic软件模拟钢板安放,Stoppa入路组的手术切口长度要比腹股沟入路组小,手术暴露时间短,术中失血量少,麻醉时间和苏醒时间短,具有统计学差异(P < 0.05)。2组患者的Matta影像学评分评价髋臼骨折复位质量无统计学意义(P > 0.05)。2组患者的髋关节Postel评分评价术后髋关节功能无统计学意义(P > 0.05)。2组患者术后并发症比较中,Stoppa入路组要明显低于腹股沟入路组,具有统计学意义(P < 0.05)。结论:3D打印导板下的钢板可以做到解剖复位和坚强内固定,Stoppa入路减少软组织损伤,降低术中出血量,更适用于3D打印导板下的钢板固定髋臼骨折。
关键词
3D建模,腹股沟入路,Stoppa入路,髋臼骨折
Comparative Study of Inguinal Approach and Stoppa Approach in the Treatment of Acetabular Fractures with 3D Printing Guide Plat
Lijian Shao
Department of Orthopedics, Hengdian Wenrong Hospital, Jinhua Zhejiang

Received: Nov. 20th, 2020; accepted: Dec. 23rd, 2020; published: Dec. 30th, 2020

ABSTRACT
Objective: To compare the effect of groin approach and Stoppa approach in the treatment of acetabular fractures with 3D printing guide plate, and to find the best surgical approach. Method: In this study, 142 patients who were admitted to our hospital from January 2012 to January 2019 were selected. All patients were treated with preoperative 3D printing technology to simulate the injury types of acetabular fractures. The plates were pre molded or customized according to the type of fracture before operation. According to the surgical approach, they were randomly divided into two groups, including 68 cases of inguinal approach group, 46 cases of male and 22 cases of female. There were 74 cases in Stoppa approach group, including 51 males and 23 females. The data of CT + 3D reconstruction and CTA of iliac vessels were collected and saved in the form of DICOM and imported into mimic software for software processing to restore acetabular fractures. At the same time, using the software of 3ds Max 2013, the fracture reduction, screw position and size were designed. The exposure time, incision length and intraoperative blood loss were counted and recorded; the quality of acetabular fracture reduction was evaluated by Matta imaging score, and the hip joint function was evaluated according to the hip Postel score. Results: There was no significant difference in general data between the two groups (P > 0.05). The length of incision in Stoppa approach group was smaller than that in groin approach group, with shorter exposure time, less blood loss, shorter anesthesia time and recovery time (P < 0.05). There was no significant difference in the quality of acetabular fracture reduction evaluated by Matta imaging score between the two groups (P > 0.05). The Postel score of hip joint in the two groups had no statistical significance (P > 0.05). In the comparison of postoperative complications between the two groups, the Stoppa approach group was significantly lower than the inguinal approach group, with statistical significance (P < 0.05). Conclusion: The plate under 3D printing guide plate can achieve anatomical reduction and rigid internal fixation. Stoppa approach can reduce soft tissue damage and reduce intraoperative blood loss. It is more suitable for plate fixation of acetabular fracture under 3D printing guide plate.
Keywords:3D Modeling, Inguinal Approach, Stoppa Approach, Acetabular Fracture

Copyright © 2020 by author(s) and Hans Publishers Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY 4.0).
http://creativecommons.org/licenses/by/4.0/


1. 引言
髋臼骨折是创伤外科常见的一种高能量损伤,具有创伤大,手术难度大,预后差等特点 [1] [2]。而这种特点是由髋臼固有的解剖结构所决定的,该处解剖位置深,血管和神经错综复杂,尤其是对于肥胖患者,手术的难度又会进一步增加,神经和血管的损伤往往是困扰外科医生的关键问题 [3] [4] [5]。而且该处骨折不规则,钢板贴合不牢,塑形困难,由此导致的手术时间延长,暴露时间延长,从而导致术中失血过多,术后并发症的发生率升高等种种问题,因此,如何正确规避血管和神经的损伤,如何根据骨折的类型做好充分的术前准备,尤其关键 [6]。随着3D打印(three dimensional print)技术引入医疗圈以来,就给这种损伤提供了一种个体化医疗的可能,而且随着社会的发展,3D打印的成本逐年降低,也为个体化医疗的发展提供进一步的推动作用 [7] [8]。本研究在3D打印技术充分术前准备的前提下,探究两种手术入路腹股沟入路和Stoppa入路与3D打印技术相结合,寻求一种最佳的组合方案,从而为临床上髋臼骨折的治疗提供一种最佳的治疗方案。
2. 资料与方法
2.1. 一般基准资料
所有的手术均由同一高年资主任医师主刀完成。选取自2012年1月~2019年1月入我院创伤外科的142例患者,所有患者均采用术前3D打印技术模拟患者髋臼骨折的损伤类型,术前根据骨折的类型对钢板进行预先塑形或者直接定制个体化钢板,由厦门大博公司提供。入组患者按照随机数字表法随机分成2组,包括腹股沟入路组和Stoppa入路组。本研究获得伦理委员会的批准许可(ZHHDYY2019-022421)。
2.2. 纳入标准
1) 骨折类型符合Letournel-Judet分型标准;2) 患者以及家属均获知情同意,签署知情同意书;3) 医从性较好,可以很好的完成随访工作。
2.3. 排除标准
1) 重度骨质疏松的高龄患者;2) 患有严重心肺功能障碍的患者,无法耐受手术;3) 未签署知情同意书的患者。
2.4. 术前准备
1) 收集患者的CT + 三维重建资料和髂血管CTA的数据,以DICOM形式保存,导入Mimic软件中,进行软件处理,对髋臼骨折进行还原。有利于医生对骨折的类型,血管的走行,骨折线的位置可以有个更加直观的概念。同时采用3ds Max 2013软件,对骨折的复位,螺钉的位置和大小进行设计。
2) 3D打印:将设计好的Mimic软件数据进行保存,以.STL格式输入到ATSmake 3D打印机中构建骨盆模型,体外定制个体化钢板模具或者对钢板进行塑形,按照预先设计的方案,对仿真模具进行钢板固定,观察是否可以在模具上进行贴合。记录螺钉的方向和长度。
2.5. 手术方法
术前1天常规灌肠和备皮,选取仰卧位,常规消毒铺巾。
1) 腹股沟入路 [9]:消毒区域为脐上10 cm水平线和过脐垂直线,患侧下肢常规消毒,方便进行下肢活动度检测,会阴备皮和消毒,常规铺巾,贴含碘保护膜,切口取自耻骨联合上方2 cm至髂前上棘连线中内2/3,钝性分离髂肌止点和斜肌腱;分离精索(圆韧带)和腹股沟神经,切断联合肌腱和腹直肌肌鞘,牵开股神经束,髂腰肌,内侧淋巴管和股动静脉。寻找闭孔动脉交通支(死亡冠)并结扎,充分暴露髋臼前柱、髂骨翼、耻骨支和四边体等结构。
2) Stoppa入路 [10]:消毒区域为脐上10 cm水平线和过两侧髂前上棘垂直线,会阴备皮和消毒,常规铺巾,贴含碘保护膜,切口取自耻骨联合上方1 cm处作长10~14 cm横切口,切开腹白线,钝性分离腹直肌,分离耻骨后间隙(Retzius间隙),寻找闭孔动脉交通支(死亡冠)并结扎,钝性分离股神经束,髂腰肌,暴露骶髂关节、坐骨大切迹、髋臼后柱以及方形区等结构。
3) 髋臼骨折的复位和固定:按照Mimic软件术前模拟对骨折的复位顺序进行,配合枪状加压复位钳、大力持骨钳等器械复位骨折,克氏针临时固定,首先解剖复位髋臼前柱,贴合预先贴合的塑形钢板,进而复位后柱和四方区,防止四方区内移和股骨头脱位。书中C臂摄片,位置理想后,逐层缝合切口。
2.6. 术后处理
术后常规使用头孢唑林钠1.5 g ivgtt bid进行抗感染治疗。术后48 h开始使用利伐沙班(拜瑞妥,10 mg/d)进行抗凝治疗,穿弹力袜,防止血栓形成。术后2天床边摄片,观察钢板位置和骨折情况。早期功能锻炼,防止术后褥疮和坠积性肺炎的发生。
2.7. 观察指标
1) 统计并记录手术显露时间、切口长度、术中出血量;床边骨盆正位平片分析术后骨折复位质量;出院及末次随访时髋关节功能评分等。
2) 利用Matta 影像学评分评价髋臼骨折复位质量 [11],术后骨折块分离最大距离 < 4 mm为优,4~10 mm 为良,11~20 mm 为可,>20 mm为差;
3) 根据髋关节Postel评分 [12] 评价髋关节功能,该评分从疼痛、行走、活动范围来对患侧髋关节进行功能评分,满分为18分,其中18分为优,15~17分为良,13~14分为可,<13分为差。
4) 术后并发症统计:包括股外侧皮神经损伤,术后腹股沟斜疝发生,膀胱损伤风险。
2.8. 统计学处理
采用SPSS 10.0软件进行统计学分析,计量资料均采用 表示,组间比较采用t检验,计数资料比较利用χ2检验,以P < 0.05为差异具有统计学意义。
3. 结果
3.1. 2组患者一般基准资料比较结果
2组患者一般基准资料比较无统计学差异(P > 0.05)。如表1。

Table 1. General baseline comparison of two groups
表1. 2组患者的一般基准情况比较
3.2. 术前准备资料
本研究将患者的CT + 三维重建资料和髂血管CTA的数据,以DICOM形式保存,导入Mimic软件中,进行软件处理,将设计好的Mimic软件数据进行保存,以.STL格式输入到ATS make 3D打印机中构建骨盆模型,观察模具上钢板的贴合情况,记录螺钉的方向和长度。如图1和图2。
 (a) Mimic软件模拟骨盆髋臼骨折;(b) Mimic软件模拟钢板安放;(c) ATS make 3D打印机打印仿真模型,安放骨盆钢板;(d) 在仿真模型上安放髋臼骨折的钢板。
(a) Mimic软件模拟骨盆髋臼骨折;(b) Mimic软件模拟钢板安放;(c) ATS make 3D打印机打印仿真模型,安放骨盆钢板;(d) 在仿真模型上安放髋臼骨折的钢板。
Figure 1. The results of the Mimic software and 3D printing model
图1. Mimic软件结果和3D打印模型结果
 (a) 腹股沟入路;(b) 腹股沟入路中术中分离子宫圆韧带;(c) Stoppa入路;(d) Stoppa入路中显露子宫圆韧带。
(a) 腹股沟入路;(b) 腹股沟入路中术中分离子宫圆韧带;(c) Stoppa入路;(d) Stoppa入路中显露子宫圆韧带。
Figure 2. The surgical approach
图2. 手术入路
3.3. 2组患者的一般手术资料
结果显示,Stoppa入路组的手术切口长度要比腹股沟入路组小,手术暴露时间短,术中失血量少,麻醉时间和苏醒时间短,具有统计学差异(P < 0.05)。如表2。
Table 2. The results of general operation data of two groups of patients
表2. 2组患者的一般手术资料比较结果
3.4. 2组患者的Matta影像学评分评价髋臼骨折复位质量
结果显示,2组患者的Matta影像学评分评价髋臼骨折复位质量无统计学意义(P > 0.05)。如表3。
Table 3. The results of Matta imaging score between the two groups
表3. 2组患者的Matta影像学评分比较结果
3.5. 2组患者髋关节Postel 评分评价术后髋关节功能
结果显示,2组患者的髋关节Postel评分评价术后髋关节功能无统计学意义(P > 0.05)。如表4。
Table 4. The Postel score and hip joint function between the two groups
表4. 2组患者的Postel评分比较术后髋关节功能
3.6. 术后2组患者的并发症比较结果
结果显示,2组患者术后并发症比较中,Stoppa入路组要明显低于腹股沟入路组,具有统计学意义(P < 0.05)。如表5。
Table 5. The results of postoperative complications between the two groups
表5. 2组患者术后并发症的比较结果
3.7. 经典病例术前和术后图片
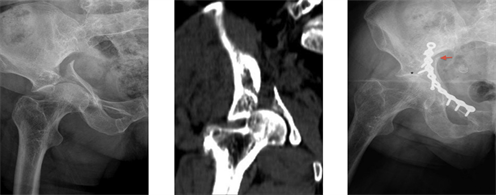
结果显示,采用腹股沟入路行骨盆髋臼骨折治疗效果满意,如图3。采用Stoppa入路行骨盆髋臼骨折治疗也可以达到满意的术后效果,如图4。
 (a) (b) (c)(a) 术前骨盆正位片;(b) 术前CT片;(c) 术后骨盆正位片。
(a) (b) (c)(a) 术前骨盆正位片;(b) 术前CT片;(c) 术后骨盆正位片。
Figure 3. A 37-year-old female patient with transverse acetabular fracture in letournel-Judet classification was treated by inguinal approach
图3. 采用腹股沟入路行骨盆髋臼骨折案例,女性,37岁,Letournel-Judet分型中髋臼横断骨折
 (a) (b)(c)(a) 术前骨盆正位片;(b) 术前CT片;(c) 术后骨盆正位片。
(a) (b)(c)(a) 术前骨盆正位片;(b) 术前CT片;(c) 术后骨盆正位片。
Figure 4. A 35-year-old male patient with acetabular fracture was treated by Stoppa approach
图4. 采用Stoppa入路行骨盆髋臼骨折案例,男性,35岁,Letournel-Judet分型中髋臼横断骨折
4. 讨论
本研究立足于临床上常见的骨盆骨折合并髋臼骨折的问题,结合3D打印技术 [13] [14],在最大程度减少肌肉,血管和神经损伤的基础上,争取髋臼骨折的解剖复位,寻找最佳的钢板固定方案,利用Mimics软件,将患者的骨盆平片,髋关节CT数据 + 3维重建数据等对髋臼骨折进行整合,然后模拟钢板的摆放位置,目的是更好的对髋臼骨折进行解剖复位,因为髋臼与下肢股骨头构成人体最大的承重关节,而且活动度最大,符合关节内骨折的标准 [15]。所以需要对骨折进行解剖复位,才可以最大程度上恢复髋关节功能。因此争取最佳的解剖复位,最小的肌肉神经损伤是本研究的特点之一。
另外本研究在3D建模前提下,探究最佳的手术方式,是本研究的特点之二。既往文献中报道 [16] [17] [18] [19],针对骨盆骨折合并髋臼骨折的治疗中,临床上可以采用的手术入路主要有腹股沟入路,高位髂腹股沟入路,Stoppa入路等,各种入路的关注点在于如何合理的暴露骨折线,以及如何有利于摆放钢板的位置。而本研究在此基础上,利用3D建模的思路,结合个体化原则,争取厦门大博公司的支持,探究针对骨盆骨折合并髋臼骨折的治疗方案,研究结果表明,将3D打印技术可以具备更好的操作性和有利于骨折线和钢板的固定,更好的做好解剖复位。本研究的病例中,均可以做到很好的贴合。充分术前准备以及术中贴合良好的优点有2个:1) 可以充分节约手术时间,从而减少手术暴露时间,进而降低手术中的出血量,降低感染概率;2) 可以做到解剖复位,尽最大可能性的恢复髋关节功能,保护髋关节。
目前,大多数研究只在于探究何种入路可以做到对骨折周围软组织的保护,那种手术入路可以对肌肉,神经等产生最小的损伤,那种入路可以取得很好的术后效果 [20]。然而,本研究认为,良好的术后效果在于如何做到骨折的解剖复位和坚强内固定,而3D打印理念指导下的钢板塑形可以做到这一点。本研究中两种手术入路,即髂腹股沟入路和Stoppa入路在Matta影像学评分中无统计学差异,结果说明,两种手术入路均可以使髋臼骨折良好复位,而良好复位的前提就是充分的术前准备。而术中切口长度,术中失血量,麻醉时间以及术后并发症的比较中,Stoppa入路要优于腹股沟入路。
综上所述,3D建模理念可以做到解剖复位和坚强内固定,Stoppa入路减少软组织损伤,降低术中出血量,适用于骨盆骨折合并髋臼骨折。
文章引用
邵莉剑. 腹股沟入路与Stoppa入路在应用3D打印导板治疗髋臼骨折的对比研究
Comparative Study of Inguinal Approach and Stoppa Approach in the Treatment of Acetabular Fractures with 3D Printing Guide Plat[J]. 医学诊断, 2020, 10(04): 236-244. https://doi.org/10.12677/MD.2020.104038
参考文献
- 1. Zhu, W., Ma, X., Gou, M., et al. (2016) 3D Printing of Functional Biomaterials for Tissue Engineering. Current Opinion in Biotechnology, 40, 103-112. https://doi.org/10.1016/j.copbio.2016.03.014
- 2. 董伊隆, 钱约男, 刘良乐, 等. 髋臼骨折不同内固定方式的生物力学稳定性研究[J]. 中国骨伤, 2018, 31(5): 420-424.
- 3. Dong, Y.L., Qian, Y.M., Liu, L.L., et al. (2018) Biomechanical Stability of Acetabular Fractures with Different Internal Fixation Methods. China Journal of Orthopaedics and Traumatology, 31, 420-424.
- 4. Lee, A.K., Wagner, B.R., Mcphillips, K., et al. (2017) Locking Compression Pilon Plate for Fixation of Comminuted Posterior Wall Acetabular Fractures: A Novel Technique. Journal of Orthopaedic Trauma, 31, e32. https://doi.org/10.1097/BOT.0000000000000675
- 5. 王雨辰, 马勇, 俞伟忠, 等. 计算机虚拟复位结合3D打印技术在髋臼骨折中的临床应用[J]. 中国骨伤, 2017, 30(7): 627-632.
- 6. Wang, Y.C., Ma, Y., Yu, W.Z., et al. (2017) Clinical Application of Computer Virtual Reduction Combined with 3D Printing Technology in Acetabular Fracture. China Journal of Orthopaedics and Traumatology, 30, 627-632.
- 7. Chui, K.H., Chan, C., Ip, K.C., et al. (2017) Three-Dimensional Navigation-Guided Percutaneous Screw Fixation for Nondisplaced and Displaced Pel-vi-Acetabular Fractures in a Major Trauma Centre. International Orthopaedics, 42, 1387-1395.
- 8. Beckmann, N.M., Chinapuvvula, N.R. and Cai, C. (2017) Association of Femoral Head and Acetabular Fractures on Computerized Tomography: Correlation with the Judet-Letournel Classification. Emergency Radiology, 24, 531-539. https://doi.org/10.1007/s10140-017-1509-3
- 9. Chanarodriguez, F., Mañanes, R.P., Rojomanaute, J., et al. (2016) 3D Surgical Printing and Pre Contoured Plates for Acetabular Fractures. Injury: International Journal of the Care of the Injured, 47, 2507-2511. https://doi.org/10.1016/j.injury.2016.08.027
- 10. Lin, X., Xiao, X., Wang, Y., et al. (2018) Biocompatibility of Bespoke 3D-Printed Titanium Alloy Plates for Treating Acetabular Fractures. BioMed Research International, 2018, Article ID: 2053486. https://doi.org/10.1155/2018/2053486
- 11. Meena, S., Sharma, P.K., Mittal, S., et al. (2017) Modified Stoppa Approach versus Ilioinguinal Approach for Anterior Acetabular Fractures; A Systematic Review and Meta-Analysis. Bulletin of Emergency and Trauma, 5, 6-12.
- 12. Verbeek, D.O., Ponsen, K.J., Van, M.H., et al. (2018) Modified Stoppa Approach for Operative Treatment of Acetabular Fractures: 10-Year Experience and Mid-Term Follow-Up. Injury: International Journal of the Care of the Injured, 49, 1137-1140. https://doi.org/10.1016/j.injury.2018.03.031
- 13. Hu, T., Xu, H., Jiang, C., et al. (2017) Treatment of Transverse with or without Posterior Wall Fractures of Acetabulum Using a Modified Smith-Petersen Combined with Kocher-Langenbeck Approach. Medical Science Monitor: International Medical Journal of Experimental & Clinical Research, 23, 2765-2774. https://doi.org/10.12659/MSM.901966
- 14. Braun, B.J., Wrona, J., Veith, N.T., et al. (2016) Predictive Value of Clinical Scoring and Simplified Gait Analysis for Acetabulum fractures. Journal of Surgical Research, 206, 405-410. https://doi.org/10.1016/j.jss.2016.08.061
- 15. Maini, L., Verma, T., Sharma, A., et al. (2018) Evaluation of Accu-racy of Virtual Surgical Planning for Patient-Specific Pre-Contoured Plate in Acetabular Fracture Fixation. Archives of Orthopaedic and Trauma Surgery, 138, 495-504. https://doi.org/10.1007/s00402-018-2868-2
- 16. Sebaaly, A., Riouallon, G., Zaraa, M., et al. (2018) Standardized Three Dimensional Computerised Tomography Scanner Reconstructions Increase the Accuracy of Acetabular Fracture Classification. International Orthopaedics, 42, 1957-1965. https://doi.org/10.1007/s00264-018-3810-5
- 17. Upex, P., Jouffroy, P. and Riouallon, G. (2017) Application of 3D Printing for Treating Fractures of Both Columns of the Acetabulum: Benefit of Pre-Contouring Plates on the Mir-rored Healthy Pelvis. Orthopaedics & Traumatology: Surgery & Research, 103, 331-334. https://doi.org/10.1016/j.otsr.2016.11.021
- 18. Zeng, C.J., Huang, W.H., Huang, H.J., et al. (2017) Laparoscopic Acetabular Fracture Fixation after Three-Dimensional Modelling and Printing. Indian Journal of Orthopaedics, 51, 620. https://doi.org/10.4103/0019-5413.214215
- 19. Gillispie, G.J., Babcock, S.N., Mcnamara, K.P., et al. (2017) Biomechanical Comparison of Intrapelvic and Extrapelvic Fixation for Acetabular Fractures Involving the Quadrilateral Plate. Journal of Orthopaedic Trauma, 31, 570-576. https://doi.org/10.1097/BOT.0000000000000963
- 20. Chui, K.H., Chan, C., Ip, K.C., et al. (2017) Three-Dimensional Navigation-Guided Percutaneous Screw Fixation for Nondisplaced and Displaced Pelvi-Acetabular Fractures in a Major Trauma Centre. International Orthopaedics, 42, 1387-1395.