设为首页
加入收藏
期刊导航
网站地图
首页
期刊
数学与物理
地球与环境
信息通讯
经济与管理
生命科学
工程技术
医药卫生
人文社科
化学与材料
会议
合作
新闻
我们
招聘
千人智库
我要投搞
办刊
期刊菜单
●领域
●编委
●投稿须知
●最新文章
●检索
●投稿
文章导航
●Abstract
●Full-Text PDF
●Full-Text HTML
●Full-Text ePUB
●Linked References
●How to Cite this Article
Asian Case Reports in
Oncology
亚洲肿瘤科病例
研究
, 2014, 3,
15-18
http://dx.doi.org/10.12677/acrpo.2014.31005
Published Online
January 2014 (http://www.hanspub.org/journal/acrpo
.html
)
Type with Somatic Cell Malignant Mediastinal Teratoma
:
A Case Report
Bo
Zhang
1
,
Wei
Cao
2
, Zhonglian
Huang
1
, Zhendong
Chen
1*
1
Oncology Department of the Second Affiliated Hospital of Anhui Medical University
,
Hefei
2
Cardiothoracic Surgery of the Second Affiliated Hospital of Anhui Medical University, Hefei
Email:
*
chenzhendong@csco.org.cn
Received: Nov
.
20
th
, 2013; revised: Dec. 4
th
, 2013; accepted: Dec. 8
th
, 2013
Copyright © 201
4 Bo Zhang
et al . This is an open acc ess article distributed under the Creative Commons Attribution License, which permits unre-
stricted use, distribution, and reproduction in any medium, provided the origin al work is properly cited. In accordance of th e Creative Commons A
t-
tribution License all Copyrights © 201
4
are reserved for Hans and the owner of the intellectual property
Bo Zhang
et al. All Copyright © 20 1
4
are
guarded by law and by Hans as a guardian.
Abstract:
Malignant mediast inal teratoma is an undifferentiated mature teratoma, wh ich is
located in the mediastinum
.
I
n clinical
,
it is very rare in China.
Such
patients mainly
had
chest tightness, shortness of breath for
space
-occupying
and
oppression symptoms caused by adjacent organs as chief complaint
s.
By image, it is hard to distinguish benign or
malignant
mediastinal ter atoma, also no t easy
to identify with other recurrent tumors
in
mediastinum
,
such as thymoma
and b
ronchial cyst
.
It
can be well determined for tumor types by invasive examination (surgical excision
or
biopsy),
pathology inspection.
In
10 years
,
there are very few clinical reports about the
mediastinal malignant teratoma
in China
,
especially the
malignant
mediastinal teratoma with somatic cell type, which i
s of
high malignant
degree
.
Patients
’
prognosis is poor
with a
short progression
-
free sur
viv
al
period. By reporting
a
case of malignant mediastinal teratoma
with somatic cell type,
we
discuss the interdisciplinary
treatment
for such
disease.
Keywords:
M alignant Mediastinal Teratoma
;
Somatic Cell
;
Interdisciplinary Treatment
伴体细胞型的纵膈恶性畸胎瘤病例报告
张
博
1
,曹
炜
2
,黄忠连
1
,陈振东
1*
1
安徽医科大学第二附属医院肿瘤科,合肥
2
安徽医科大学第二附属医院心胸外科,合肥
Email:
*
chenzhendong@csco.org.cn
收稿日期:
2013
年
11
月
20
日;修回日期:
2013
年
12
月
4
日;录用日期:
2013
年
12
月
8
日
摘
要:
纵膈恶性畸胎瘤是占位于纵膈内的一种未分化成熟的畸胎瘤,临床上较少见。此类病患主要以胸闷,
气短等因占位压迫邻近器官造成的症状为主诉。在影像学表现上很难与良性纵膈畸胎瘤区分,也不易与纵膈内
其他常发肿瘤鉴别如胸腺瘤,支气管囊肿等。通过侵袭性检查
(
手术、穿刺活检
)
可明确,并在病理检验后确诊具
体类型。近十年内有关纵膈恶性畸胎瘤的报告较少,特别是伴体细胞型的纵膈恶性畸胎瘤,其恶性程度高,治
疗效果较差,病患预后不良,生存期很短。本病例报道一例伴体细胞型的纵膈恶性畸胎瘤,借此讨论此类肿瘤
的综合治疗方案。
关键词:
恶性畸胎瘤;
体细胞
;综合治疗
*
通讯作者。
OPEN ACCESS
15
伴体细胞型的纵膈恶性畸胎瘤病例报告
1.
引言
恶性畸胎瘤约占纵膈畸胎瘤
10%
,为未成熟性畸
胎瘤,伴体细胞型的纵膈畸胎瘤更极为少见。近年来
发现的伴体细胞型纵膈恶性畸胎瘤的影像学表现与
良性纵膈畸胎瘤类似,以囊性纵膈内占位为主,病患
也多以肿瘤压迫所致症状如胸闷,气促为主诉。但是
此类型肿瘤治疗效果差,复发率高,病患生存期短
[1
-3]
,
很难追踪临床治疗效果,此病的治疗方案一直在讨论
之中。本文报道了一例伴体细胞型纵膈恶性畸胎瘤病
例,并借此病例对此类肿瘤的术后治疗进行讨论及总
结。
2.
病历摘要
患者,女,
45
岁,汉族,安徽舒城,从事化工制
品劳动
12
年。
患者于
2013
年
8
月出现活动后胸闷、气喘一周
于安徽医科大学第二附属医院,停经
8
月否认呼吸系
统及心血管系统疾病史;;无肿瘤家族史;入院体检:
神清,步入病房,呼吸不促,皮肤巩膜无黄染及出血
点,颈软,浅表淋巴结未及肿大,胸廓无畸,听诊双
肺呼吸音清,未闻及明显干湿罗音。心尖搏动位置正
常,心率
78
次
/
分,律齐,各瓣膜区未及明显杂音,
腹部查体未见异常,四肢肌力正常,神经检查
(-)
。血
常规、尿常规、大便常规、肝肾功能无异常。
2013
年
8
月
26
日当地医院
胸部
B
超提示左侧胸腔囊实性占位,
考虑畸胎瘤可能。
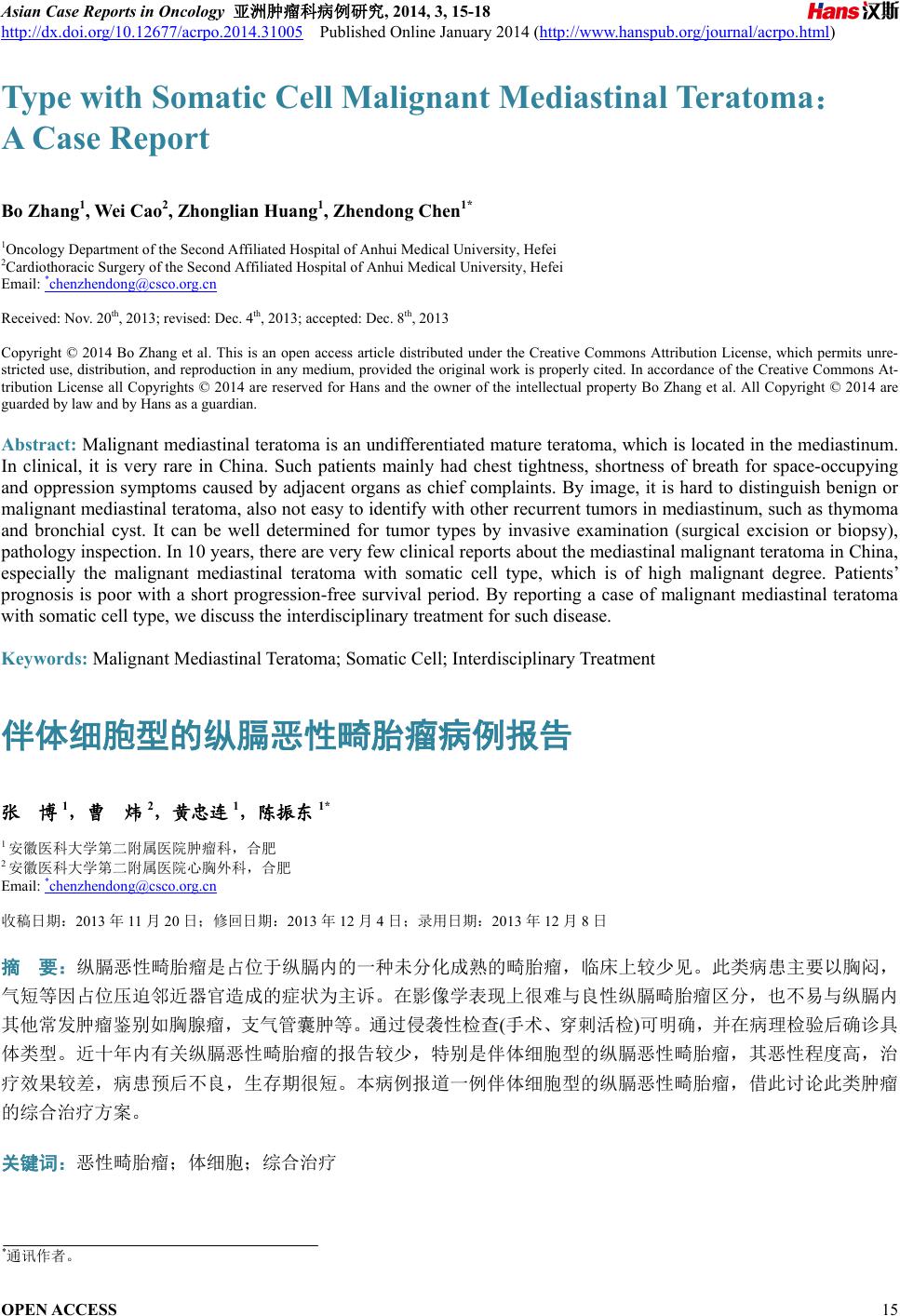
2013
年
09
月
03
日本院胸部增强
CT
:左侧纵隔囊性占位,畸胎瘤可
能性大
(
图
1)
。
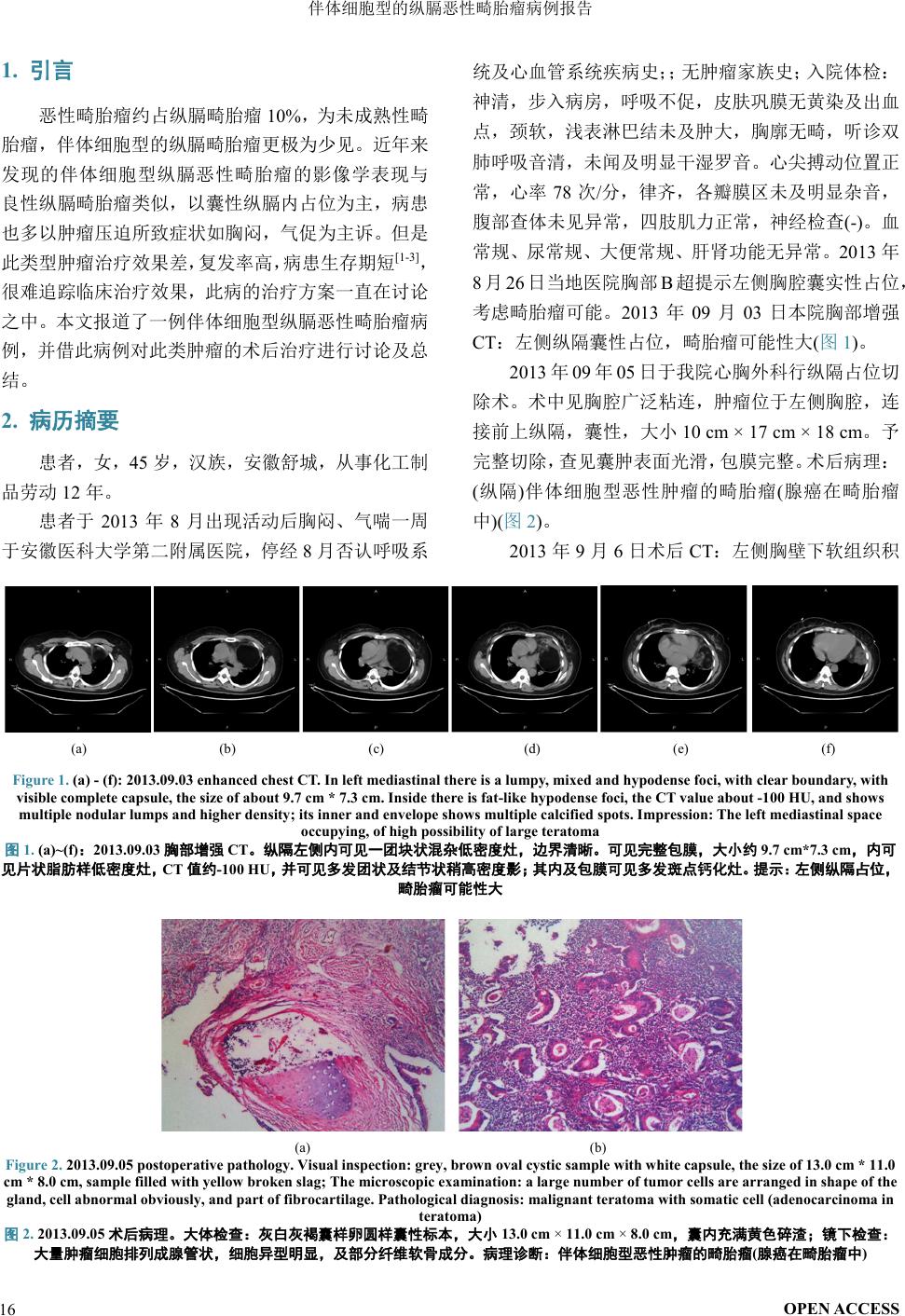
2013
年
09
年
05
日于我院心胸外科行纵隔占位切
除术
。术中
见胸腔广泛粘连,肿瘤位于左侧胸腔,连
接前上纵隔,囊性,大小
10
cm
×
17
cm
×
18
cm
。予
完整切除,查见囊肿表面光滑,包膜完整。术后病理:
(
纵隔
)
伴体细胞型恶性肿瘤的畸胎瘤
(
腺癌在畸胎瘤
中
)(
图
2)
。
2013
年
9
月
6
日术后
CT
:左侧胸壁下软组织积
(a) (b) (c)
(d) (e) (f)
Figure 1. (a) - (f)
:
2013.09.03 enhanced chest CT. In left mediastinal there is a lumpy
,
mixed and hypodense
foci
, with
clear boundary
, with
visible complete capsule, the size of about
9.7
cm * 7.3 cm. Inside there is
fat
-like hypodense
foci, the
CT value about -100 HU, and shows
multiple n
odular lumps and higher density; its inner and envelope shows multiple calcified spots
.
Impression: The left mediastinal space
occupying
,
of high possibility of large teratoma
图
1.
(a)~(
f)
:
2013.09.03
胸部增强
CT
。纵隔左侧内可见一团块状混杂低密度灶,边界清晰。可见完整包膜,大小约
9.7
cm*7.3 cm
,内可
见片状脂肪样低密度灶,
CT
值约
-100
HU
,并可见多发团状及结节状稍高密度影;其内及包膜可见多发斑点钙化灶。提示:左侧纵隔占位,
畸胎瘤可能性大
(a)
(b)
Figure 2. 2013.09.05 postoperative pathology
.
Visual inspection: grey, brown oval cystic sample with white capsule, the size of 13.0 cm * 11.0
cm * 8.0 cm, sample filled with yellow broken slag; The microscopic examination: a large number of tumor cells are arranged in shape of the
gland, cell abnormal obviously, and part of fibrocartilage. Pathological diagnosis: malignant teratoma with somatic cell (adenocarcinoma in
teratoma)
图
2.
2013.09.05
术后病理。大体检查:灰白灰褐囊样卵圆样囊性标本,大小
13. 0 cm
×
11.0 cm
×
8.0 cm
,囊内充满黄色碎渣;镜下检查:
大量肿瘤细胞排列成腺管状,细胞异型明显,及部分纤维软骨成分。病理诊断:伴体细胞型恶性肿瘤的畸胎瘤
(
腺癌在畸胎瘤中
)
OPEN ACCESS
16
伴体细胞型的纵膈恶性畸胎瘤病例报告
(a) (b) (c)
(d) (e) (f)
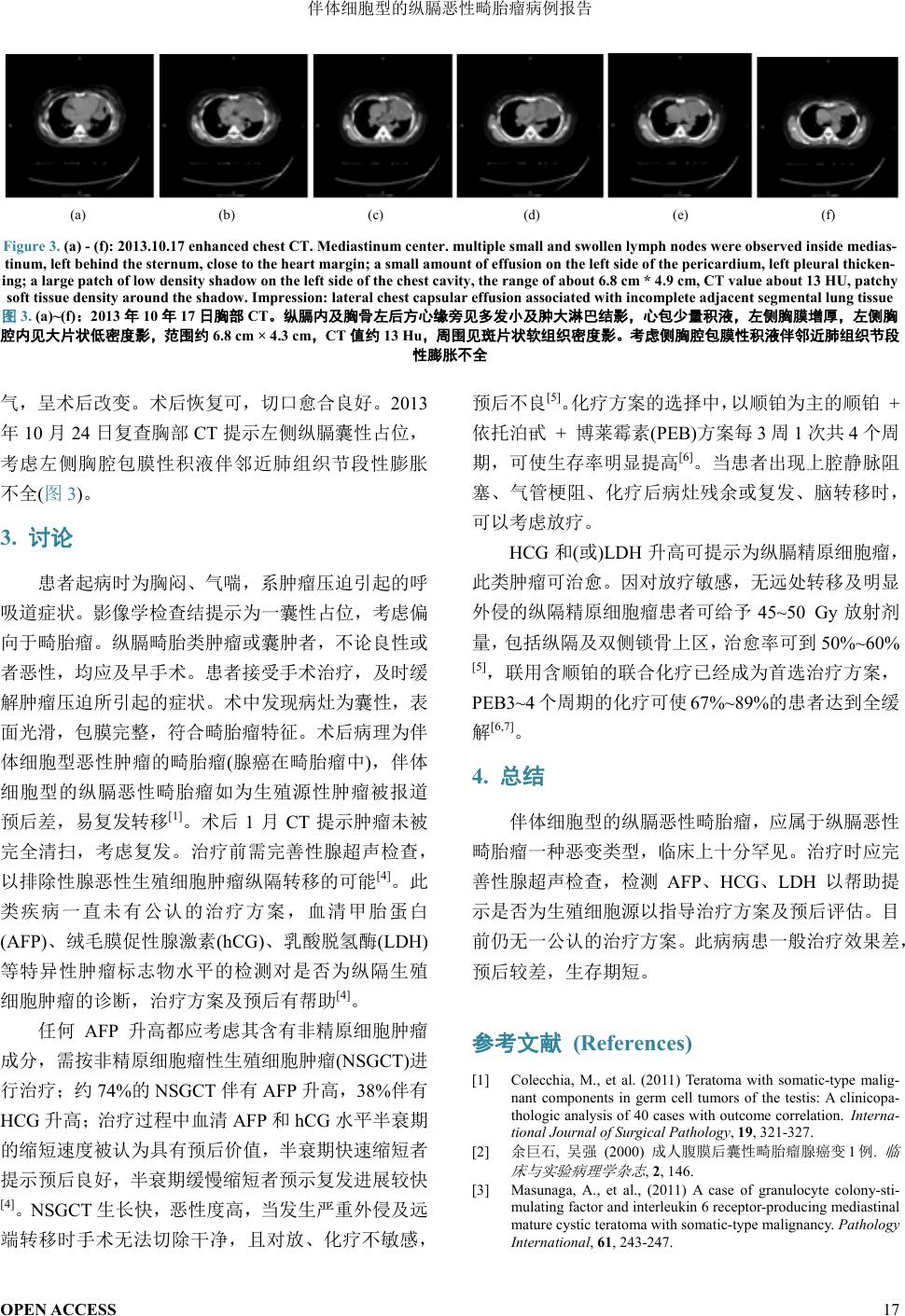
Figure 3.
(a)
-
(f):
2013.10.17 enhanced chest CT
.
Mediastinum center. multiple small and swollen lymph nodes were observed inside medias-
tinum, left behind the sternum, close to the
hear t marg in
;
a small amount of effusion on the left side of the pericardium, left pleural thicken-
ing
;
a large patch of low density shadow on the left side of the chest cavity, the range of about 6.8 cm * 4.9 cm, CT value about 13
HU
, patchy
soft tissue density around the shadow. Impression: lateral chest capsular effusion associated with incomplete adjacent segmental lung tissue
图
3.
(a)
~
(f)
:
2013
年
10
年
17
日胸部
CT
。纵膈内及胸骨左后方心缘旁见多发小及肿大淋巴结影,心包少量积液,左侧胸膜增厚,左侧胸
腔内见大片状低密度影,范围约
6
.8 cm
× 4.3 cm
,
CT
值约
13 Hu
,周围见斑片状软组织密度影。考虑侧胸腔包膜性积液伴邻近肺组织节段
性膨胀不全
气,呈术后改变。术后恢复可,切口愈合良好。
2013
年
10
月
24
日复查胸部
CT
提示左侧纵膈囊性占位,
考虑左侧胸腔包膜性积液伴邻近肺组织节段性膨胀
不全
(
图
3)
。
3.
讨论
患者起病时为胸闷、气喘,系肿瘤压迫引起的呼
吸道症状。影像学检查结提示为一囊性占位,考虑偏
向于畸胎瘤。纵膈畸胎类肿瘤或囊肿者,不论良性或
者恶性,均应及早手术。患者接受手术治疗,及时缓
解肿瘤压迫所引起的症状。术中发现病灶为囊性,表
面光滑,包膜完整,符合畸胎瘤特征。术后病理为伴
体
细胞型恶性肿瘤的畸胎瘤
(
腺癌在畸胎瘤中
)
,伴体
细胞型的纵膈恶性畸胎瘤如为生殖源性肿瘤被报道
预后差,易复发转移
[1]
。术后
1
月
CT
提示肿瘤未被
完全清扫,考虑复发。治疗前需完善性腺超声检查,
以排除性腺恶性生殖细胞肿瘤纵隔转移的可能
[4]
。此
类疾病一直未有公认的治疗方案,血清
甲胎蛋白
(AFP)
、绒毛膜促性腺激素
(
hCG
)
、乳酸脱氢酶
(LDH)
等特异性肿瘤标志物水平的检测对是否为纵隔生殖
细胞肿瘤的诊断,治疗方案及预后
有帮助
[4]
。
任何
AFP
升高都应考虑其
含有非精原细胞肿瘤
成分,需按非精原细胞瘤性生殖细胞肿瘤
(NSGCT)
进
行治疗;约
74
%
的
NSGCT
伴有
AFP
升高,
38
%
伴有
H
CG
升高;治疗过程中血清
AFP
和
hCG
水平半衰期
的缩短速度被认为具有预后价值,半衰期快速缩短者
提示预后良好,半衰期缓慢缩短者预示复发进展较快
[4]
。
NSGCT
生长快,恶性度高,当发生严重外侵及远
端转移时手术无法切除干净,且对放、化疗不敏感,
预后不良
[5]
。化疗方案的选择中,以顺铂为主的
顺铂
+
依托泊甙
+
博莱霉素
(
PEB
)
方案每
3
周
1
次共
4
个周
期,可使生存率明显提高
[6]
。当患者出现上腔静脉阻
塞、气管梗阻、化疗后病灶残余或复发、脑转移时,
可以考虑放疗。
H
CG
和
(
或
)
LDH
升高
可提示为纵膈精原细胞瘤,
此类肿瘤可治愈。因对放疗敏感,无远处转移及明显
外侵的纵隔精原细胞瘤患者可给予
45
~50
Gy
放射剂
量,包括纵隔及双侧
锁骨
上区,治愈率可到
50%
~60%
[5]
,联用含顺铂的联合化疗已经成为首选治疗方案,
PEB3~4
个
周期的化疗可使
67
%~
89%
的患者达到全缓
解
[6,7]
。
4.
总结
伴体细胞型的纵膈恶性畸胎瘤,应属于纵膈恶性
畸胎瘤一种恶变类型,临床上十分罕见。治疗时应完
善性腺超声检查,检测
AFP
、
HCG
、
LDH
以帮助提
示是否为生殖细胞源以指导治疗方案及预后评估。目
前仍无一公认的治疗方案。此病病患一般治疗效果差,
预后较差,生存期短。
参考文献
(References)
[1]
Colecchia, M., et al.
(2011)
Teratoma with somatic
-
type malig
-
nant components in germ cell tumors of the testis:
A
clinicopa-
thologic analysis of 4 0 cases with outcome correlation.
Interna-
tional Journal of Surgical P athology
,
19
, 321
-327.
[2]
余巨石
,
吴强
(2000)
成人腹膜后囊性畸胎瘤腺癌变
1
例
.
临
床与实验病理学杂志
,
2
, 146.
[3]
Masunaga, A., et al.,
(2011)
A case of granulocyte colony
-sti-
mulating factor and interleukin 6 receptor
-
producing mediastinal
mature cystic teratoma with somatic-
type malignancy.
Pathology
International
,
61
, 243-247.
OPEN ACCESS
17
伴体细胞型的纵膈恶性畸胎瘤病例报告
[4]
Bokemeyer, C., et al.
(2002)
Extragonadal germ cell tumors o
f
the mediastinum and retroperitoneum:
Results
from an interna-
tional analysis.
Journal of Clinical Oncology
,
20
,
1864-1873.
[5]
Fizazi, K., et al.
(1998
)
Initial management of primary medias-
tinal seminoma:
Radiotherapy
or cisp latin
-
based chemotherapy?
European Jour nal of Cancer
,
34
, 347-352.
[6]
Anthoney, D.A., et al.
(2004)
Bleomycin, vincristine, cispla-
tin/bleomycin, etoposide, cisp latin che motherapy:
An alternating,
dose intense regimen producing promising results in untreated
patients with intermediate or poor
prognosis malignant germ
-cell
tumours.
British Journal of Cancer
,
90
, 601-606.
[7]
Motzer, R.J., et al.
(2000)
Sequential dose
-
intensive paclitaxel,
ifosfamide, carboplatin, and etoposide salvage therapy for germ
cell tumor patients.
Journal of Clinical Oncolo
gy
,
18
,
1173-
11
80
.
OPEN ACCESS
18