 Asian Case Reports in Vascular Medicine 亚洲心脑血管病例研究, 2012, 1, 10-14 http://dx.doi.org/10.12677/acrvm.2012.11003 Published Online November 2012 (http://www.hanspub.org/journal/acrvm.html) The Effect of Attentional Bias Modification on the Cardiovascular Stress Reactivity* Wenjie Duan Department of Cross-Culture and Psychology Research, Cultural Development Research Institute in Chongqing Municipality, Chongqing Email: wjtuan@gmail.com Received: Sep. 19th, 2012; revised: Sep. 24th, 2012; accepted: Sep. 29th, 2012 Abstract: Although with worldwide progress of modern medicine, there have been a lot of the centralized and deep re- searches about precipitating factors of cardiovascular disease, data published by WHO shows the morbidity rate of cardio- vascular disease in the global scope has increased, so this highlights that under the background of the whole development of modern medicine, it is necessary to employ the physiological-psychological-social medical model to find a new method to break through traditional biochemical monitoring index, which can prevent, identify and intervene the individual who will develop into the risk of cardiovascular disease before the organic disease formed. Previous researches have suggested that, in the face of the pressure source, individual system will react to it, which is called cardiovascular stress reactivity, and this kind of long-term, inappropriate physiology reaction can eventually lead to organic lesion, namely the generation of cardiovascular disease. This paper is to utilize literature review to explore the following subjects in two dimensions of theory and practice: correct individual attention bias to change the cognitive process of negative information (such as the pressure source), so as to reduce the cardiovascular stress reactivity produced by individual when facing pressure, eventu- ally to reduce improper physiol ogy react ion and the ri sk of developing i nto cardiovascul ar disease. Keywords: Attentional Bias; Attentional Bias Modification; Cardiovascular Stress Reactivity 注意偏向修正对心血管应激反应的影响* 段文杰 重庆市文化发展研究会,跨文化与心理研究部,重庆 Email: wjtuan@gmail.com 收稿日期:2012 年9月19 日;修回日期:2012 年9月24 日;录用日期:2012 年9月29 日 摘 要:尽管随着世界范围内现代医学的进步,对心血管疾病的诱发因素进行了大量、集中、深入的研究,但 据WHO 公布的数据说明心血管疾病的患病率在全球范围还是不断增高,因此这突出表明在整体医学不断发展 的背景下,有必要采用生理–心理–社会医学模式来发现突破传统生化指标监测的新方法,在器质性疾病形成 以前,起到预防、识别和干预有发展成心血管疾病风险的个人。以往研究表明,个体在面对压力源时,心血管 会对压力产生相应反应,被称为心血管应激反应性,而这种长期的、不恰当的生理反应会最终导致器质性病变, 即心血管疾病的产生。因此本文通过文献回顾,提出可在理论与实践两个维度进行探究的新命题:通过对个体 注意偏向的修正改变其对负面信息(如压力源)的认知加工过程,从而降低个体在面对压力时产生的心血管应激反 应性,最终达到减轻不恰当生理反应,降低发展成心血管疾病风险的目的。 关键词:注意偏向;注意偏向修正;心血管应激反应 *基金项目:本文受教育部哲学社会科学研究重大课题攻关项目(批准文号:10JZD0005)资助。 Copyright © 2012 Hanspub 10  注意偏向修正对心血管应激反应的影响 Copyright © 2012 Hanspub 11 1. 引言 世界卫生组织于近日公布了心血管疾病(Cardio- vascular Disease, CVD)最新研究结果,截至 2011 年9 月,心血管疾病仍然是全球范围内造成死亡的最主要 原因,即与其它任何原因相比,心血管疾病每年造成 的死亡数最多、死亡率最高。仅在 2008 年,估计有 17.3 万人死于心血管疾病,占全球所有死亡人数 的 30%,预计到2030 年,这一数字将增长到23.6 万。 目前,全世界对心血管疾病的危险因素研究集中 在生化指标领域,主要有:胰岛素抵抗(Insulin Re- sistance)[1-5]、炎症(Inflammation)[6-8] 、生理止血 (Hemostasis)[9-11]、心脏自主神经功能(Cardiac Auto- nomic Control)[12-16]、抑 郁 症 (Depression)[17-20]、高血压 (Hypertension)[21-24]、血脂异常(Dyslipidemia)[25-28]和肥 胖(Obesity) [29-31]等。 从上述研究结果及世界卫生组织公布的预测数 据来看,尽管全世界在控制心血管疾病的危险因素方 面取得了长足进步,但心血管疾病的患病率在全球范 围还是不断增高。这突出表明需要有突破传统生化指 标监测的新方法,在器质性疾病形成以前,起到预防、 识别和治疗有发展成心血管疾病风险的个人。 2. 研究现状及其价值 2.1. 个体心理层面 部分研究者将视线转向了个体心理层面,A型人 格(Type A)[32]和D型人格(Type D)[33-36]被认为与心血 管疾病的发病率有极高的相关性,但人格属于比较稳 定的心理特质,短时间内不会被轻易改变,因此一般 情况下只能起到识别心血管疾病发病高危人群的作 用。 2.2. 认知层面 于是近十年来,不少学者开始从认知取向角度来 探讨导致心血管疾病的因素。心理压力和情感压力所 引起的心血管反应性(Cardiovascular Reactivity)被认 为是“注意和认知领域”增加心血管患病风险的最主 要潜在因素[37]。经常性暴露于压力源下,并产生过分 夸张的或不恰当的反应性倾向会在心血管疾病重要 的调控系统(Regulatory Systems)中产生外显的变化 (Allostatic Changes),如血压调节、脂质和胰岛素代谢、 炎症及生理止血等,这种长期的、不恰当的生理反应 会最终导致器质性病变,即心血管疾病的产生。在面 对压力源时,心血管对压力所产生的反应性被称为心 血管应激反应性(Cardiovascular Stress Reactivity),一 般来说,以测量接受刺激(可以是生理刺激,也可以是 引起心理压力的心理任务)前后心率(Heart Rate,HR)、 收缩压(Systolic Blood Pressure,SBP) 和舒张压 (Diastolic Blood Pressure,DBP)之间的差异表示。 然而,面对同一种压力源时,不同的人会有不同 的反应,其原因在于个体在加工信息时具有不同的认 知偏向(包括注意偏向、记忆偏向、解释偏向等),其 在绝大多数时候都不利于人们更好的认识与解决问 题、适应环境,例如对负性情绪刺激的选择性注意与 焦虑易感性提升相关[38-40]。在面对“压力源”进行认 知加工的一系列过程中,注意无疑是最先出现的阶 段,更有研究者发现焦虑障碍、情感障碍、摄食障碍、 物质成瘾、暴力攻击、慢性疼痛等患者对威胁信息的 注意分配与常人不同:相对于中性刺激,他们会更快、 更早对相应威胁或相关刺激表现出不同的注意分配, 即注意偏向(Attentional Bias),甚至先于意识[41-43]。进 一步的研究表明,注意偏向不仅仅是一些心理疾病所 伴随的现象或症状,而且是心理疾病产生、维持和复 发的原因[44-46]。对这一命题一致共识进行逻辑演绎, 我们认为:可以通过对个体注意偏向的修正改变其对 负面信息(如压力源)的认知加工过程,从而降低个体 在面对压力时产生的心血管应激反应性,最终达到减 轻不恰当生理反应,降低发展成心血管疾病风险的目 的。 2.3. 注意偏向修正的应用价值 近年来,在西方临床治疗领域,已有不少研究者 在进行注意偏向修正(Attentional Bias Modification, ABM)的研究与实践[47]。这种修正程序源于焦虑症中 与威胁有关注意偏向的研究,以基于计算机的注意培 训教程内隐地改变焦虑症患者的有偏注意模式 (Biased Attentional Patterns)。目前运用得比较多且成 熟的修正程序有两种,改版的点/视觉探测任务和改版 的视觉搜索任务,而对注意偏向修正的效果评估可以 采用各种评估注意偏向的实验范式,如改版的 Stroop 任务、点/视觉探测任务、空间提示任务等,这些任务 用不同的指标来评估注意偏向的改变[48],其原理图如 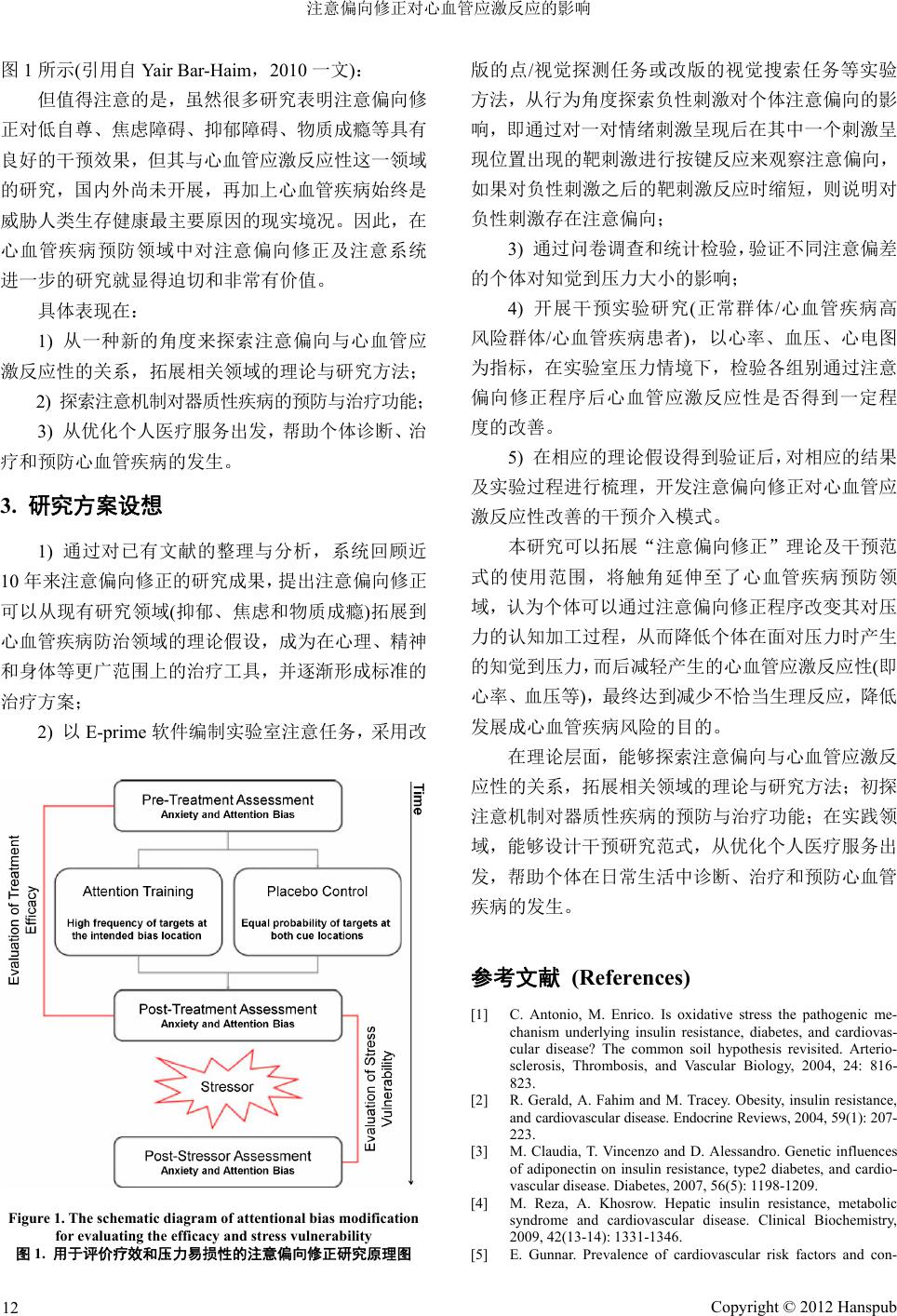 注意偏向修正对心血管应激反应的影响 图1所示(引用自 Yair Bar-Haim,2010 一文): 但值得注意的是,虽然很多研究表明注意偏向修 正对低自尊、焦虑障碍、抑郁障碍、物质成瘾等具有 良好的干预效果,但其与心血管应激反应性这一领域 的研究,国内外尚未开展,再加上心血管疾病始终是 威胁人类生存健康最主要原因的现实境况。因此,在 心血管疾病预防领域中对注意偏向修正及注意系统 进一步的研究就显得迫切和非常有价值。 具体表现在: 1) 从一种新的角度来探索注意偏向与心血管应 激反应性的关系,拓展相关领域的理论与研究方法; 2) 探索注意机制对器质性疾病的预防与治疗功能; 3) 从优化个人医疗服务出发,帮助个体诊断、治 疗和预防心血管疾病的发生。 3. 研究方案设想 1) 通过对已有文献的整理与分析,系统回顾近 10 年来注意偏向修正的研究成果,提出注意偏向修正 可以从现有研究领域(抑郁、焦虑和物质成瘾)拓展到 心血管疾病防治领域的理论假设,成为在心理、精神 和身体等更广范围上的治疗工具,并逐渐形成标准的 治疗方案; 2) 以E-prime 软件编制实验室注意任务,采用改 Figure 1. The schematic diagram of attentional bias modification for evaluating t he efficacy and stress vulnerability 图1. 用于评价疗效和压力易损性的注意偏向修正研究原理图 版的点/视觉探测任务或改版的视觉搜索任务等实验 方法,从行为角度探索负性刺激对个体注意偏向的影 响,即通过对一对情绪刺激呈现后在其中一个刺激呈 现位置出现的靶刺激进行按键反应来观察注意偏向, 如果对负性刺激之后的靶刺激反应时缩短,则说明对 负性刺激存在注意偏向; 3) 通过问卷调查和统计检验,验证不同注意偏差 的个体对知觉到压力大小的影响; 4) 开展干预实验研究(正常群体/心血管疾病高 风险群体/心血管疾病患者),以心率、血压、心电图 为指标,在实验室压力情境下,检验各组别通过注意 偏向修正程序后心血管应激反应性是否得到一定程 度的改善。 5) 在相应的理论假设得到验证后,对相应的结果 及实验过程进行梳理,开发注意偏向修正对心血管应 激反应性改善的干预介入模式。 本研究可以拓展“注意偏向修正”理论及干预范 式的使用范围,将触角延伸至了心血管疾病预防领 域,认为个体可以通过注意偏向修正程序改变其对压 力的认知加工过程,从而降低个体在面对压力时产生 的知觉到压力,而后减轻产生的心血管应激反应性(即 心率、血压等),最终达到减少不恰当生理反应,降低 发展成心血管疾病风险的目的。 在理论层面,能够探索注意偏向与心血管应激反 应性的关系,拓展相关领域的理论与研究方法;初探 注意机制对器质性疾病的预防与治疗功能;在实践领 域,能够设计干预研究范式,从优化个人医疗服务出 发,帮助个体在日常生活中诊断、治疗和预防心血管 疾病的发生。 参考文献 (References) [1] C. Antonio, M. Enrico. Is oxidative stress the pathogenic me- chanism underlying insulin resistance, diabetes, and cardiovas- cular disease? The common soil hypothesis revisited. Arterio- sclerosis, Thrombosis, and Vascular Biology, 2004, 24: 816- 823. [2] R. Gerald, A. Fahim and M. Tracey. Obesity, insulin resistance, and cardiovascular disease. Endocrine Reviews, 2004, 59 (1): 207- 223. [3] M. Claudia, T. Vincenzo and D. Alessandro. Genetic influences of adiponectin on insulin resistance, type2 diabetes, and cardio- vascular disease. Diabetes, 2007, 56(5): 1198-1209. [4] M. Reza, A. Khosrow. Hepatic insulin resistance, metabolic syndrome and cardiovascular disease. Clinical Biochemistry, 2009, 42(13-14): 1331-1346. [5] E. Gunnar. Prevalence of cardiovascular risk factors and con- Copyright © 2012 Hanspub 12  注意偏向修正对心血管应激反应的影响 centration of C-reactive protein in Type D personality persons without cardiovascular disease. European Journal of Preventive Cardiology, 2011, 18(3): 504-509. [6] P. Mathieu, I. Lemieux and J. P. Després. Obesity, inflammation, and cardiovascular risk. Clinical Pharmacology & Therapeutics, 2010, 87(4): 407-416. [7] Z. X. Wang, N. Tomohiro. Inflammation, a link between obesity and cardiovascular disease. Mediators of Inflammation, 2010, 2010: 17. [8] M. Elena, C. S. Crowson, H. M. Kremers, V. L. Roger, P. D. Fitz-Gibbon, T. M. Therneau and S E. Gabrie. Lipid paradox in rheumatoid arthritis: the impact of serum lipid measures and systemic inflammation on the risk of cardiovascular disease. Clinical and Epidemiological Re sea rch , 2011, 70(3): 482-487. [9] T. Lisman, S. H. Caldwell, A. K. Burroughs, P. G. Northup, M. Senzolo, R. T. Stravitz, A. Tripodi, J. F. Trotter, D. C. Valla and R. J. Porte. Hemostasis and thrombosis in patients with liver disease: The ups and downs. Journal of Hepatology, 2010, 53(2): 362-371. [10] E. Brodin, T. Vikan, J. B. Hansen and J. Svartberg. Testosterone, hemostasis, and cardiovascular diseases in men. Seminars in Thrombosis and Hemostasis, 2011, 37(1): 87-94. [11] S. Yende, G. D’Angelo, F. Mayr, J. A. Kellum, L. Weissfeld, A. M. Kaynar, T. You ng, K. Irani and D C. Angus. Elevated hemo- stasis markers after pneumonia increases one-year risk of all-cause and cardiovascular deaths. Hemostasis Markers and Pneumonia Mortality, 2011, 6(8): e22847. [12] R. Pop-Busui, G. W. Evans, H. C. Gerstein, V. Fonseca, J. L. Fleg, B. J. Hoogwerf, S. Genuth, R. H. Grimm, M. A. Corson and R. Prineas. Effects of cardiac autonomic dysfunction on mortality risk in the action to control cardiovascular risk in dia- betes (ACCORD) trial. Diabetes Care, 2010, 33(7): 1578-1584. [13] P. Paolo, J. Stevo. The role of cardiac autonomic function in hypertension and cardiovascular disease. Current Hypertension Reports, 2007, 11(3): 199-205. [14] X. Wang, X. Ding, S. Su, Z. Li, H. Riese, J. F. Thayer, et al. Genetic influences on heart rate variability at rest and during stress. Psychophysiology. 2009, 46(3): 458-465. [15] N. Kupper, G. Willemsen, D. Posthuma, D. De Boer, D. Boomsma and E. J. De Geus. A genetic analysis of ambulatory cardiorespi- ratory coupling. Psychophysiology, 2005, 42(2): 202-212. [16] N. Kupper, G. Willemsen, D. I. Boomsma and E. J. De Geus. Heritability of indices for cardiac contractility in ambulatory re- cordings. Journal of Cardiovascular Electrophysiology, 2006, 17(8): 877-883. [17] Andrew, H, Kemp, Quintana D S, Gray M A. Is heart rate vari- ability reduced in depression without cardiovascular disease? Biological Psychiatry, 2011, 69(4): e3-e4. [18] A. C. Phillips. Blunted cardiovascular reactivity relates to de- pression, obesity, and self-reported health. Biological Psychol- ogy, 2011, 86(2): 106-113. [19] A. J. Grippo, A. K. Johnson. Stress, depression and cardiovas- cular dysregulation: A review of neurobiological mechanisms and the integration of research from preclinical disease models. Stress, 2009, 12(1): 1-21. [20] P. F. Sullivan, M. C. Neale and K. S. Kendler. Genetic epidemi- ology of major depression: Review and meta-analysis. American Journal of Psychiatry, 2000, 157(10): 1552-1562. [21] A. M. Thompson, T. Hu, C. L. Eshelbrenner, K. Reynolds, J. He and L. A. Bazzano. Antihypertensive treatment and secondary prevention of cardiovascular disease events among persons without hypertension. Journal of the American Medical Associa- tion, 2011, 305(9), 913-922. [22] Buxtona, O M, Marcelli E. Short and long sleep are positively associated with obesity, diabetes, hypertension, and cardiovas- cular disease among adults in the United States. Social Science & Medicine, 2010, 71(5): 1027-1036. [23] D. M. Mannino, D. Thorn, A. Swensen and F. Holguin. Preva- lence and outcomes of diabetes, hypertension and cardiovascular disease in COPD. European Respiratory Journal, 2008, 32(4): 962-969. [24] C. M. Champagne. Magnesium in hypertension, cardiovascular disease, metabolic syndrome, and other conditions: A review. Nutrition in Clinical Practice, 2008, 23(2): 142-151. [25] A. G. Olsson. Laropiprant plus niacin for dyslipidemia and pre- vention of cardiovascular disease. Expert Opinion on Pharma- cotherapy, 2010, 11(10): 1715-1726. [26] M. J. Chapmana, J. S. Redfernc, M. E. McGovernd and P. Giral. Niacin and fibrates in atherogenic dyslipidemia: Pharmacother- apy to reduce cardiovascular risk. Pharmacology & Therapeutics, 2010, 126(3): 314-345. [27] J. Genest, et al. Canadian cardiovascular society/Canadian guidelines for the diagnosis and treatment of dyslipidemia and prevention of cardiovascular disease in the adult—2009 recom- mendations. Canadian Journal of Cardiology, 2009, 25(10): 567- 579. [28] D. Maccubbin, et al. Flushing profile of extended-release nia- cin/laropiprant versus gradually titrated niacin extended-release in patients with dyslipidemia with and without ischemic cardio- vascular disease. The American Journal of Cardiology, 2009, 104(1): 74-81. [29] C. J. Lavie, R. V. Milani and H. O. Ventura. Obesity and cardio- vascular disease: Risk factor, paradox, and i mpact of weight loss. Journal of the American College of Cardiology, 2009, 53(21): 1925-1932. [30] S. S. Martin, A. Qasim and M. P. Reilly. Leptin resistance: A possible interface of inflammation and metabolism in obe- sity-related cardiovascular disease. Journal of the American Col- lege of Cardiology, 2008, 52(15): 1201-1210. [31] G. M. Reaven. Insulin resistance: The link between obesity and cardiovascular disease. Medical Clinics of North America, 2011, 95(5): 875-892. [32] 姚如珍. 人格特征与心身疾病[J]. 临床心身疾病杂志, 2006, 12(1). [33] F. Mols, J. Denollet. Type D personality in the general popula- tion: A systematic review of health status, mechanisms of dis- ease, and work-related problems. Mols and Denollet Health and Quality of Life Outcomes, 2010, 8: 9. [34] N. Kupper, J. Denollet, E. J. De Geus, D. I. Boomsma and G. Willemsen. Heritability of type-D personality. Psychosomatic Medicine, 2007, 69(7): 675-681. [35] 瞿云中,黄彦科, 姚树桥. D型人格量表用于心血管病人群的 信效度[J]. 中国临床心理学杂志, 2009, 17(4): 452-456. [36] 张勇, 张亚林, 邹韶红, 李恒芬. D型人格量表在儿童少年情 绪障碍患者中的信度效度研究. 中国行为医学科学, 2006, 15(8): 757-759. [37] T. W. Kamarck, W. R. Lovallo. Cardiovascular reactivity to psychological challenge: Conceptual and measurement consid- erations. Psychosomatic Medicine, 2003, 65(1): 9-21. [38] A. Mathews, C. MacLeod. Cognitive approaches to emotion and emotional disorder s. Annual Review of Psychology, 1994, 45(1): 25-50. [39] A. Mathews, C. MacLeod. Cognitive vulnerability to emotional disorders. Annual Review of Clinical Psychology, 2005, 1: 167- 195. [40] A. C. Puliafico, P. C. Kendall. Threat-related attentional bias in anxious youth: A review. Clinical Child and Family Psychology Review, 2006, 9(3): 162-180. [41] T. Dalgleish, F. N. Watts. Biases of attention and memory in disorders of anxiety and depression. Clinical Psychology Review, 1990, 10(5): 589-604. [42] L. Sharpe, B. F. Dear and L. Schrieber. Attentional biases in chronic pain associated with rheumatoid arthritis: Hypervigi- lance or difficulties disengaging? The Journal of Pain: Official Journal of the American Pain Society, 2009, 10(3): 329. [43] E. Smeets, A. Roefs, E. Van Furth and A. Jansen. Attentional bias for body and food in eating disorders: Increased distraction, speeded detection, or both? Behaviour Research and Therapy, 2008, 46(2): 229-238. [44] S. Hayes, C. R. Hirsch, G. Krebs and A. Mathews. The effects of modifying interpretation bias on worry in generalized anxiety Copyright © 2012 Hanspub 13  注意偏向修正对心血管应激反应的影响 Copyright © 2012 Hanspub 14 disorder. Behaviour Research and Therapy, 2010, 48(3): 171- 178. [45] C. MacLeod, E. Rutherford, L. Campbell, G. Ebsworthy and L. Holker. Selective attention and emotional vulnerability: Assess- ing the causal basis of their association through the experimental manipulation of attentional bias. Journal of Abnormal Psychol- ogy, 2002, 111(1): 107-123. [46] A. M. Waters, J. S. Valvoi. Attentional bias for emotional faces in paediatric anxiety disorders: An investigation using the emo- tional go/no go task. Journal of Behavior Therapy and Experi- mental Psychiatry, 2009, 40(2): 306-316. [47] Y. Bar-Haim, D. Lamy, L. Pergamin, M. J. Bakermans-Kra- nenburg and M. H. Van IJzendoorn. Threat-related attentional bias in anxious and nonanxious individuals: A meta-analytic study. Psychological Bulletin, 2007, 133(1): 1-24. [48] J. M. Cisler, E. H. W. Koster. Mechanisms of attentional biases towards threat in the anxiety disorders: An integrative review. Clinical Psychology Review, 2010, 30(2): 203-216. |