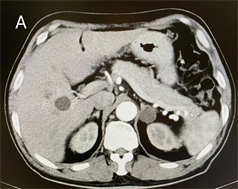
患者男,60岁,因情绪激动后出现胸闷、憋气半年余,伴有心慌、头晕、头痛收住我院心血管内科,既往高血压病史13年,规律服用“缬沙坦氨氯地平片”降压,血压控制不佳,最高为200/100 mmHg,“蛛网膜下腔出血颅内动脉瘤栓塞术后”10年,“右眼视网膜脱离”病史半年。否认吸烟饮酒史、心血管疾病及早发性高血压病家族史。入院检查心率65次/分,血压155/99 mmHg,一般情况及常规查体阴性,检验检查结果示血钾1.6 mmol/L,血钠147.8 mmol/L,尿液分析示PH 6.0,血浆醛固酮水平立位511 pg/mL、卧位655 pg/mL均升高,血浆肾素活性立位0 ng/mL/hr、卧位0 ng/mL/hr均降低,醛固酮/肾素活性比值(ARR)立位51.1、卧位65.5均升高,肾上腺CT动态增强扫描示双侧肾上腺见低密度结节影,考虑肾上腺皮质腺瘤所致的原发性醛固酮增多症,然后转泌尿外科行后腹腔镜下左肾上腺切除术,术后病理诊断为肾上腺皮质腺瘤,术后2周随访血浆醛固酮、血钾、血钠等生化指标水平均在正常范围,血压正常。
A 60-year-old male patient was admitted to the Department of Cardiovascular Medicine of our hos-pital because of chest tightness and suffocation for more than half a year after emotional agitation, accompanied by palpitation, dizziness and headache. He has a history of hypertension for 13 years and has been regularly taking “valsartan amlodipine tablets” for hypotensive for many years. His blood pressure has never been well controlled during the medication, with the highest value being 200/100 mmHg, with 10 years after intracranial aneurysm embolization for subarachnoid hemor-rhage, and half a year after retinal detachment in the right eye. The patient denied smoking and drinking history, family history of cardiovascular disease and early onset hypertension. On admis-sion, heart rate was 65 times/min, blood pressure was 155/99 mmHg, general condition and con-ventional physical examination were negative. The results of blood potassium and blood sodium were 1.6 mmol/L and 147.8 mmol/L, respectively. Urine analysis showed PH 6.0, and plasma al-dosterone levels increased in vertical position 511 pg/mL and recubitus position 655 pg/mL re-spectively. The plasma renin activity was decreased by 0 ng/mL/hr in vertical position and 0 ng/mL/hr in recubitus position, and the aldosterone/renin activity ratio (ARR) was increased by 51.1 in vertical position and 65.5 in recubitus position. Dynamic enhanced adrenal CT scan showed low- density nodular opacity in both adrenal glands, which was considered as primary aldosteron-ism caused by adrenal cortical adenoma. Then, the patient was transferred to the urology depart-ment for retroperitoneal laparoscopic left adrenal gland resection, which was pathologically diag-nosed as adrenal cortical adenoma. The plasma aldosterone, blood potassium, blood sodium and other biochemical indexes were all in the normal range and blood pressure was normal 2 weeks af-ter surgery.
原发性醛固酮增多症,肾上腺腺瘤,高血压,低血钾, Primary Aldosteronism Adrenal Adenoma High Blood Pressure Hypokalemia摘要
A Case of Primary Aldosteronism Misdiagnosed for Many Years<sup> </sup>
Mengyao Shi, Guirong Sun*
Department of Clinical Laboratory, The Affiliated Hospital of Qingdao University, Qingdao Shandong
Received: Apr. 11th, 2022; accepted: May 6th, 2022; published: May 13th, 2022
ABSTRACT
A 60-year-old male patient was admitted to the Department of Cardiovascular Medicine of our hospital because of chest tightness and suffocation for more than half a year after emotional agitation, accompanied by palpitation, dizziness and headache. He has a history of hypertension for 13 years and has been regularly taking “valsartan amlodipine tablets” for hypotensive for many years. His blood pressure has never been well controlled during the medication, with the highest value being 200/100 mmHg, with 10 years after intracranial aneurysm embolization for subarachnoid hemorrhage, and half a year after retinal detachment in the right eye. The patient denied smoking and drinking history, family history of cardiovascular disease and early onset hypertension. On admission, heart rate was 65 times/min, blood pressure was 155/99 mmHg, general condition and conventional physical examination were negative. The results of blood potassium and blood sodium were 1.6 mmol/L and 147.8 mmol/L, respectively. Urine analysis showed PH 6.0, and plasma aldosterone levels increased in vertical position 511 pg/mL and recubitus position 655 pg/mL respectively. The plasma renin activity was decreased by 0 ng/mL/hr in vertical position and 0 ng/mL/hr in recubitus position, and the aldosterone/renin activity ratio (ARR) was increased by 51.1 in vertical position and 65.5 in recubitus position. Dynamic enhanced adrenal CT scan showed low-density nodular opacity in both adrenal glands, which was considered as primary aldosteronism caused by adrenal cortical adenoma. Then, the patient was transferred to the urology department for retroperitoneal laparoscopic left adrenal gland resection, which was pathologically diagnosed as adrenal cortical adenoma. The plasma aldosterone, blood potassium, blood sodium and other biochemical indexes were all in the normal range and blood pressure was normal 2 weeks after surgery.
Keywords:Primary Aldosteronism, Adrenal Adenoma, High Blood Pressure, Hypokalemia
石梦瑶,孙桂荣. 误诊多年的原发性醛固酮增多症1例A Case of Primary Aldosteronism Misdiagnosed for Many Years[J]. 临床医学进展, 2022, 12(05): 3855-3860. https://doi.org/10.12677/ACM.2022.125557
参考文献ReferencesWang, L., Li, N., Yao, X., et al. (2017) Detection of Secondary Causes and Coexisting Diseases in Hypertensive Patients: OSA and PA Are the Common Causes Associated with Hypertension. BioMed Research International, 2017, Article ID: 8295010. <br>https://doi.org/10.1155/2017/8295010Mosso, L., Carvajal, C., González, A., et al. (2003) Primary Aldosteronism and Hy-pertensive Disease. Hypertension, 42, 161-165. <br>https://doi.org/10.1161/01.HYP.0000079505.25750.11Kogika, M.M. and de Morais, H.A. (2017) A Quick Reference on Hypokalemia. Veterinary Clinics of North America: Small Animal Practice, 47, 229-234. <br>https://doi.org/10.1016/j.cvsm.2016.10.010中华医学会内分泌学分会. 原发性醛固酮增多症诊断治疗的专家共识(2020版) [J]. 中华内分泌代谢杂志, 2020, 36(9): 727-736.张诗婷. 双侧肾上腺占位的诊治进展[J]. 中国微创外科杂志, 2018, 24(4): 349-353.
<br>https://doi.org/10.3969/j.issn.1009-6604.2018.04.016Williams, T.A., Lenders, J.W.M., Mulatero, P., et al. (2017) Out-comes after Adrenalectomy for Unilateral Primary Aldosteronism: An International Consensus on Outcome Measures and Analysis of Remission Rates in an International Cohort. The Lancet Diabetes & Endocrinology, 5, 689-699. <br>https://doi.org/10.1016/S2213-8587(17)30135-3Patel, S., Rauf, A., Khan, H. and Abu-Izneid, T. (2017) Ren-in-Angiotensin-Aldosterone (RAAS): The Ubiquitous System for Homeostasis and Pathologies. Biomedicine & Pharmacotherapy, 94, 317-325.
<br>https://doi.org/10.1016/j.biopha.2017.07.091Bothou, C., Beuschlein, F. and Spyroglou, A. (2020) Links between Aldoste-rone Excess and Metabolic Complications: A Comprehensive Review. Diabetes & Metabolism, 46, 1-7. <br>https://doi.org/10.1016/j.diabet.2019.02.003Gyamlani, G., Headley, C.M., Naseer, A., Valaulikar, G.S. and Geraci, S.A. (2016) Primary Aldosteronism: Diagnosis and Management. The American Journal of the Medical Sciences, 352, 391-398.
<br>https://doi.org/10.1016/j.amjms.2016.06.015Feigin, V.L., Lawes, C.M., Bennett, D.A. and Anderson, C.S. (2003) Stroke Epidemiology: A Review of Population- Based Studies of Incidence, Prevalence, and Case-Fatality in the Late 20th Century. The Lancet Neurology, 2, 43-53.
<br>https://doi.org/10.1016/S1474-4422(03)00266-7Briet, M. and Schiffrin, E.L. (2013) Vascular Actions of Aldosterone. Journal of Vascular Research, 50, 89-99.
<br>https://doi.org/10.1159/000345243钱婧雨, 刘向祎. 醛固酮检测方法及临床应用进展[J]. 中华检验医学杂志, 2019, 42(12): 1072-1077.
<br>https://doi.org/10.3760/cma.j.issn.1009-9158.2019.12.018Stowasser, M., Ahmed, A.H., Pimenta, E., Taylor, P.J. and Gor-don, R.D. (2012) Factors Affecting the Aldosterone/ Renin Ratio. Hormone and Metabolic Research, 44, 170-176. <br>https://doi.org/10.1055/s-0031-1295460